Quality Improvement Charts
An implementation of statistical process control charts for R
Jacob Anhøj
2026-07-02
Source:vignettes/qicharts2.Rmd
qicharts2.RmdThe qicharts2 package contains two main functions for
analysis and visualisation of data for continuous quality improvement:
qic() and paretochart().
qic() provides a simple interface for constructing
statistical process control (SPC) charts for time series data.
paretochart() constructs Pareto charts from categorical
variables.
Statistical Process Control is not about statistics, it is not about “process-hyphen-control”, and it is not about conformance to specifications. […] It is about the continual improvement of processes and outcomes. And it is, first and foremost, a way of thinking with some tools attached.
Donald J. Wheeler. Understanding Variation, 2. ed., p 152
This vignette will teach you the easy part of SPC, the
tools, as implemented by qicharts2 for R. I strongly
recommend that you also study the way of thinking, for example
by reading Wheeler’s excellent book.
Installation
Install stable version from CRAN:
install.packages('qicharts2')Or install development version from GitHub:
devtools::install_github('anhoej/qicharts2', build_vignettes = TRUE)Your first run and control charts
Load qicharts2 and generate some random numbers to play
with:
# Load qicharts2
library(qicharts2)
# Lock random number generator to make examples reproducible.
set.seed(19)
# Generate 24 random numbers from a normal distribution.
y <- rnorm(24)Make a run chart:
qic(y)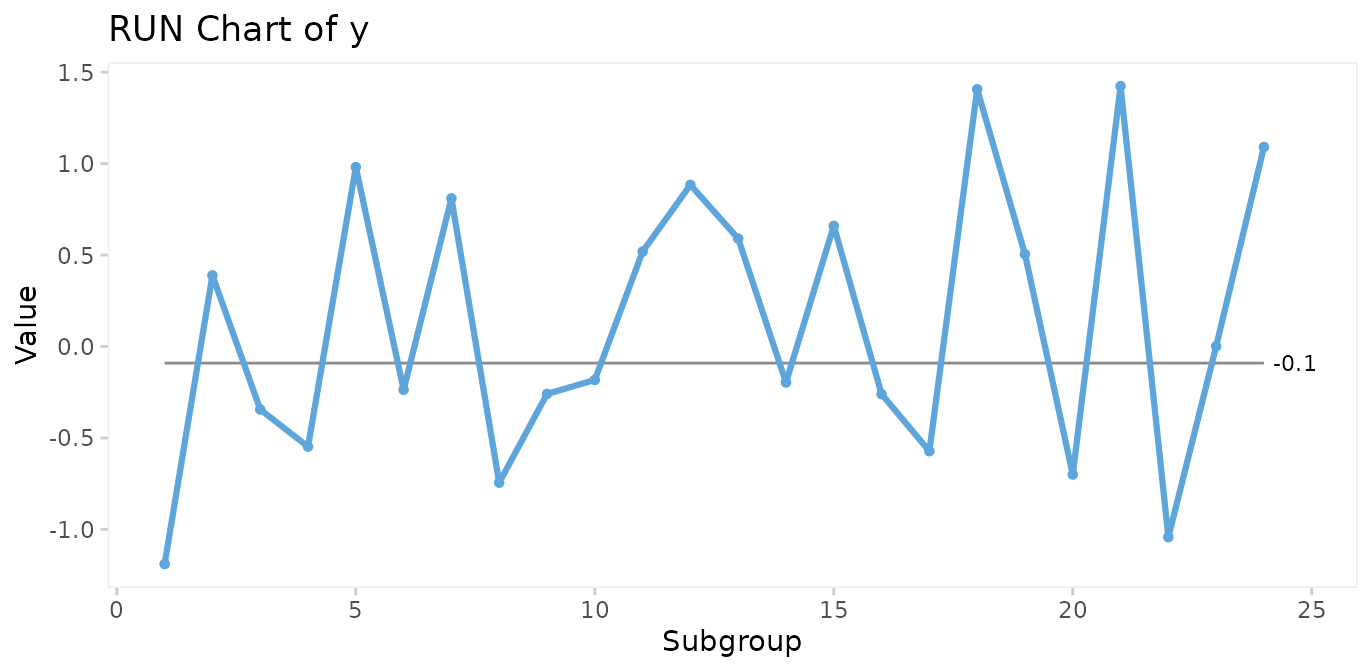
Make an I control chart:
qic(y, chart = 'i')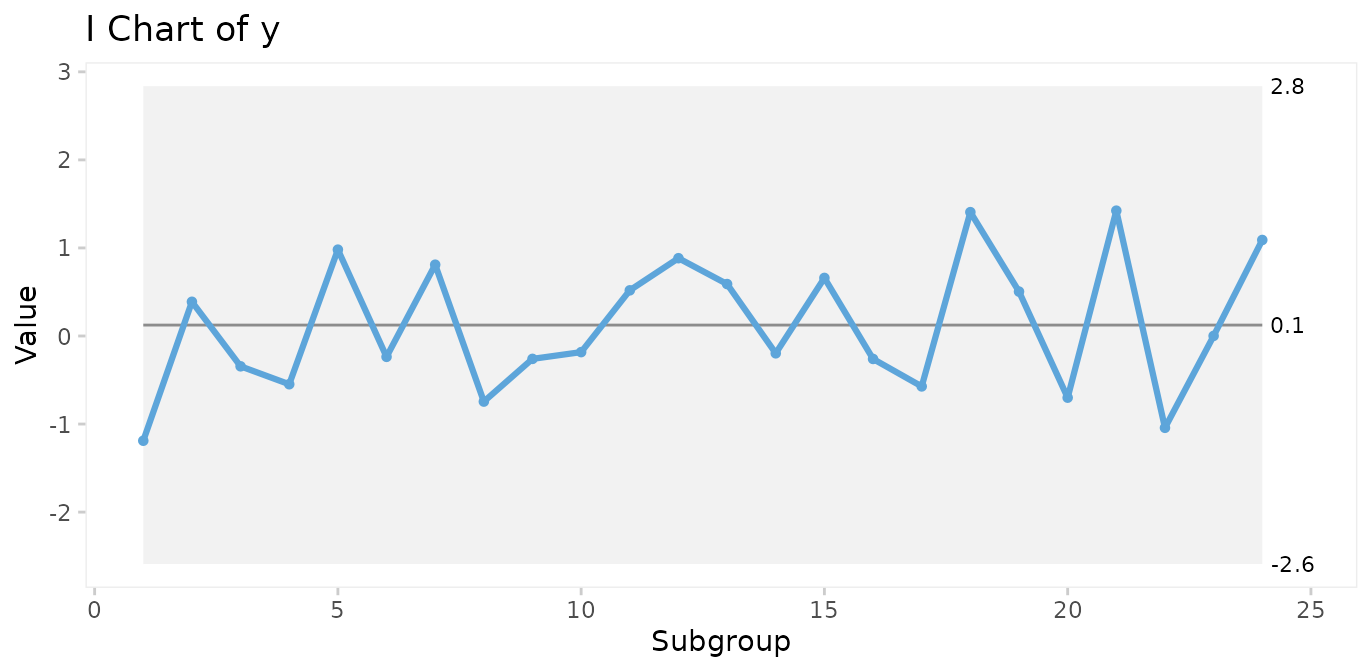
Run charts and control charts are point-and-line graphs showing measures or counts over time. A horizontal line represents the process centre expressed by either the median (run charts) or the mean (control charts). In addition, control charts visualise the limits of the natural variation inherent in the process. Because of the way these limits are computed, they are often referred to as 3-sigma limits (see Appendix 1). Other terms for 3-sigma limits are control limits and natural process limits.
Understanding variation
SPC is the application of statistical thinking and statistical tools to continuous quality improvement. Central to SPC is the understanding of process variation over time.
The purpose of analysing process data is to know when a change occurs so that we can take appropriate action. However, numbers may change even if the process stays the same (and vice versa). So how do we distinguish changes in numbers that represent change of the underlying process from those that are essentially noise?
Walther A. Shewhart, who founded SPC, described two types of variation, chance cause variation and assignable cause variation. Today, the terms common cause and special cause variation are commonly used.
Common cause variation
is also called natural/random variation or noise,
is present in all processes,
is caused by phenomena that are always present within the system,
makes the process predictable within limits.
Special cause variation
is also called non-random variation or signal,
is present in some processes,
is caused by phenomena that are not normally present in the system,
makes the process unpredictable.
A process will be said to be predictable when, through the use of past experience, we can describe, at least within limits, how the process will behave in the future.
Donald J. Wheeler. Understanding Variation, 2. ed., p 153
The overall purpose of SPC charts is to tell the two types of variation apart.
Testing for special cause variation
As expected from random numbers, the previous run and control charts exhibit common cause variation. Special cause variation, if present, may be found by statistical tests to identify patterns in data that are unlikely to be the result of pure chance.
Shewhart’s 3-sigma rule
Shewhart devised one test to identify special cause variation, the 3-sigma rule, which signals if one or more data points fall outside the 3-sigma limits. The 3-sigma rule is effective in detecting larger (> 2SD) shifts in data.
# Simulate a special cause to y in the form of a large, transient shift of 4 standard deviations.
y[22] <- 4
qic(y, chart = 'i')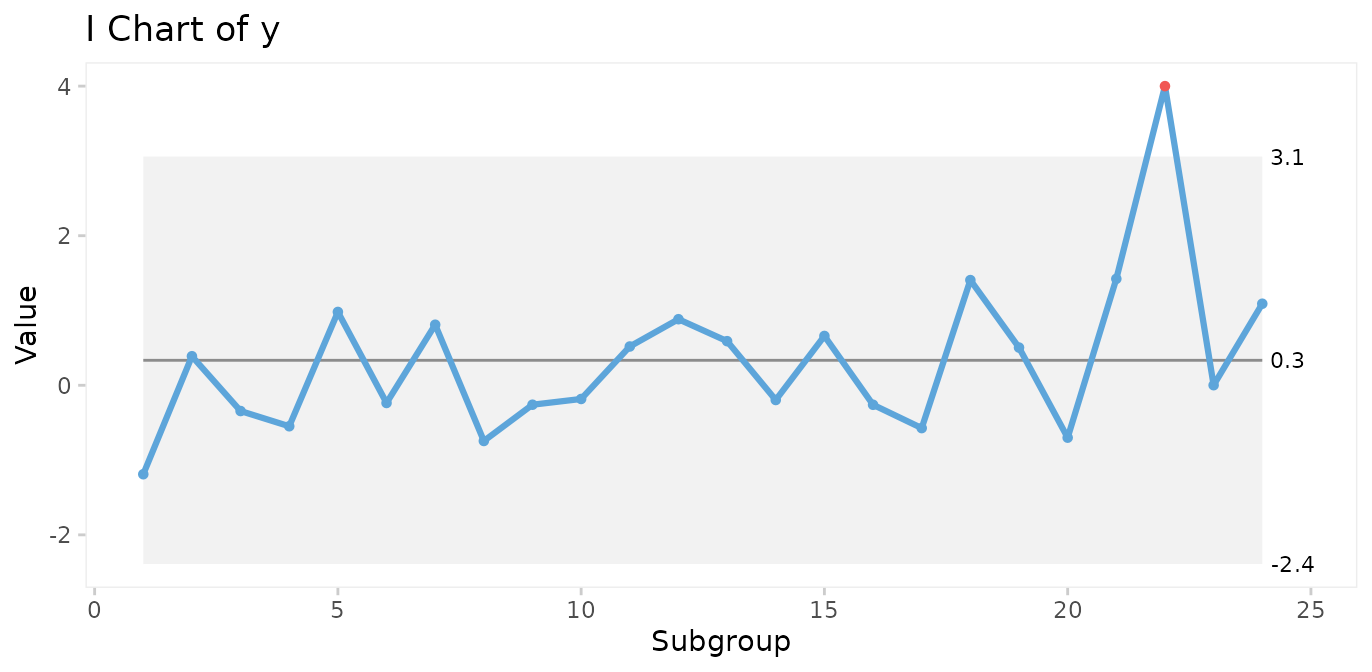
However, minor to moderate shifts may go unnoticed by the 3-sigma rule for long periods of time.
# Simulate a special cause to y in the form of a moderate, persistent shift of 2 standard deviations.
y[13:24] <- rnorm(12, mean = 2)
qic(y, chart = 'i')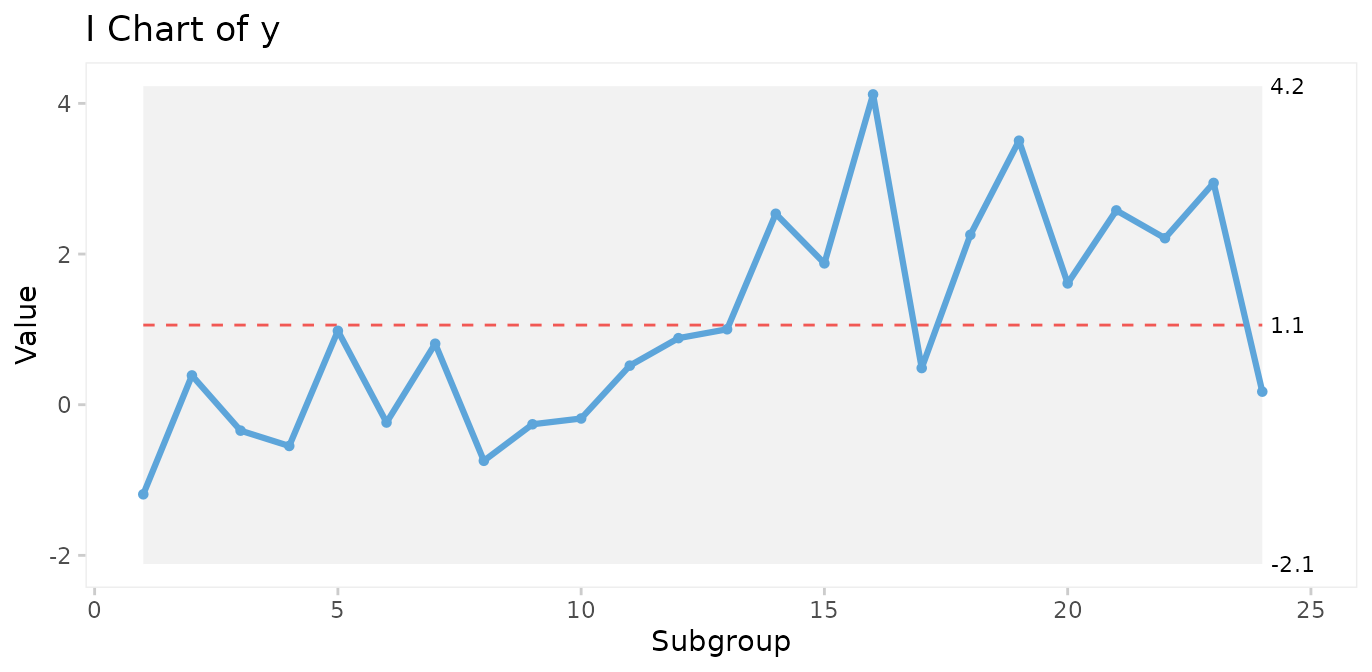
Therefore, many additional tests have been proposed to increase the sensitivity to non-random variation.
It is important to realise that while it may be tempting to apply more tests in order to increase the sensitivity of the chart, more test will increase the risk of false signals, thereby reducing the specificity of the chart. The choice of which and how many tests to apply is therefore critical.
The Western Electric rules
The best known tests for non-random variation are probably the Western Electric Rules described in the Statistical Quality Control Handbook (Western Electric Company 1956). The WE rules consist of four simple tests that can be applied to control charts by visual inspection and are based on the identification of unusual patterns in the distribution of data points relative to the control and centre lines.
One or more points outside of the 3-sigma limits (Shewhart’s original 3-sigma rule).
Two out of three successive points beyond a 2-sigma limit (two thirds of the distance between the centre line and the control line).
Four out of five successive points beyond a 1-sigma limit.
A run of eight successive points on one side of the centre line.
The WE rules have proven their worth during half a century. One thing to notice is that the WE rules are most effective with control charts that have between 20 and 30 data points. With fewer data points, they lose sensitivity (more false negatives), and with more data points they lose specificity (more false positives).
The Anhøj rules
The least known tests for non-random variation are probably the Anhøj
rules, proposed and validated by me in two recent publications (Anhøj 2014, Anhøj 2015). The
Anhøj rules are the core of qicharts2, and consist of two
tests that are based solely on the distribution of data points in
relation to the centre line:
Unusually long runs: A run is one or more consecutive data points on the same side of the centre line. Data points that fall on the centre line neither break nor contribute to the run. The upper 95% prediction limit for longest run is approximately (rounded to the nearest integer), where is the number of useful data points. For example, in a run chart with 24 data points a run of more than
round(log2(24) + 3)= 8 would suggest a shift in the process.Unusually few crossings: A crossing is when two consecutive data points are on opposite sides of the centre line. In a random process, the number of crossings has a binomial distribution, . The lower 5% prediction limit for number of crossings is found using
qbinom(p = 0.05, size = n - 1, prob = 0.5). Thus, in a run chart with 24 useful data points, fewer thanqbinom(0.05, 24 - 1, 0.5)= 8 crossings would suggest that the process is shifting.
Critical values for longest runs and number of crossings for 10 – 100 data points are tabulated in Appendix 2.
Apart from being comparable in sensitivity and specificity to WE rules 2-4 with 20-30 data points, the Anhøj rules have some advantages:
They do not depend on sigma limits and thus are useful as stand-alone rules with run charts.
They adapt dynamically to the number of available data points, and can be applied to charts with as few as 10 and up to indefinitely many data points without losing sensitivity and specificity.
In the previous control chart, a shift of 2 standard deviations was introduced halfway through the process. While the shift is too small to be picked up by the 3-sigma rule, both Anhøj rules detect the signal. The longest run includes 13 data points (upper limit = 8), and the number of crossings is 4 (lower limit = 8). Note that the shift is also picked up by WE rule 4.
Non-random variation found by the Anhøj rules is visualised by
qic() using a red and dashed centre line.
The parameters of the analysis are available using the
summary() function on a qic object. See
?summary.qic for details.
# Save qic object to o
o <- qic(y, chart = 'i')
# Print summary data frame
summary(o)
#> facet1 facet2 part n.obs n.useful longest.run longest.run.max n.crossings
#> 1 1 1 1 24 24 13 8 4
#> n.crossings.min runs.signal aLCL aLCL.95 CL aUCL.95 aUCL
#> 1 8 1 -2.114884 -1.057559 1.057091 3.171742 4.229067
#> sigma.signal
#> 1 0Many additional tests for special cause variation have been proposed
since Shewhart invented the 3-sigma rule, and many tests are currently
being used. However, the more tests that are applied to the analysis,
the higher the risk of false signals. qicharts2 takes a
conservative approach by applying only three tests, the 3-sigma rule and
the two Anhøj rules. That means that a signal from qic()
most likely represents a significant change in the underlying
process.
Choosing the right control chart
By default, qic() produces run charts. To make a control
chart, the chart argument must be specified.
While there is only one type of run chart, there are many types of control charts. Each type uses an assumed probability model to compute the 3-sigma limits.
qic() includes eleven control charts.
| Chart | Description | Assumed distribution |
|---|---|---|
| Charts for measures | ||
| I | Individual measurements | Gaussian |
| MR | Moving ranges of individual measurements | Gaussian |
| Xbar | Sample means | Gaussian |
| S | Sample standard deviations | Gaussian |
| T | Time between rare events | Exponential |
| Charts for counts | ||
| C | Defect counts | Poisson |
| U | Defect rates | Poisson |
| U’ | U chart using Laney’s correction for large sample sizes | Mixed |
| P | Proportion of defectives | Binomial |
| P’ | P chart using Laney’s correction for large sample sizes | Mixed |
| G | Opportunities between rare events | Geometric |
I recommend to always begin any analysis with the “assumption free” run chart. If the Anhøj rules find non-random variation, it makes no sense to compute 3-sigma limits based on assumptions regarding the location and dispersion of data, because these figures are meaningless when one or more shifts have already been identified.
Over the years, I have developed an increasing affection for the much-neglected run chart: a time plot of your process data with the median drawn in as a reference (yes, the median – not the average). It is “filter No. 1” for any process data and answers the question: “Did this process have at least one shift during this time period?” (This is generally signaled by a clump of eight consecutive data points either all above or below the median.)
If it did, then it makes no sense to do a control chart at this time because the overall average of all these data doesn’t exist. (Sort of like: If I put my right foot in a bucket of boiling water and my left foot in a bucket of ice water, on average, I’m pretty comfortable.)
Davis Balestracci. Quality Digest 2014
Case 1: Patient harm
The gtt dataset contains data on patient harm during
hospitalisation. Harm is defined as any unintended physical injury
resulting from treatment or care during hospitalisation and not a result
of the disease itself. The Global Trigger Tool is a methodology for
detection of adverse events in hospital patients using a retrospective
record review approach. Each month a random sample of 20 patient records
is reviewed and the number of adverse events and patient days found in
the sample are counted. See ?gtt for details.
head(gtt)
#> admission_id admission_dte discharge_dte month days harms E
#> 1 1 2010-01-02 2010-01-03 2010-01-01 2 0 <NA>
#> 2 2 2009-12-24 2010-01-06 2010-01-01 14 2 Pressure ulcer
#> 3 3 2009-12-28 2010-01-07 2010-01-01 11 0 <NA>
#> 4 4 2010-01-05 2010-01-08 2010-01-01 4 0 <NA>
#> 5 5 2010-01-05 2010-01-08 2010-01-01 4 0 <NA>
#> 6 6 2010-01-05 2010-01-11 2010-01-01 7 0 <NA>
#> F G H I
#> 1 <NA> <NA> <NA> <NA>
#> 2 Gastrointestinal <NA> <NA> <NA>
#> 3 <NA> <NA> <NA> <NA>
#> 4 <NA> <NA> <NA> <NA>
#> 5 <NA> <NA> <NA> <NA>
#> 6 <NA> <NA> <NA> <NA>Run chart of adverse events per 1000 patient days
qic(month, harms, days,
data = gtt,
multiply = 1000,
title = 'Patient harm',
ylab = 'Adverse events per 1000 patient days',
xlab = 'Month')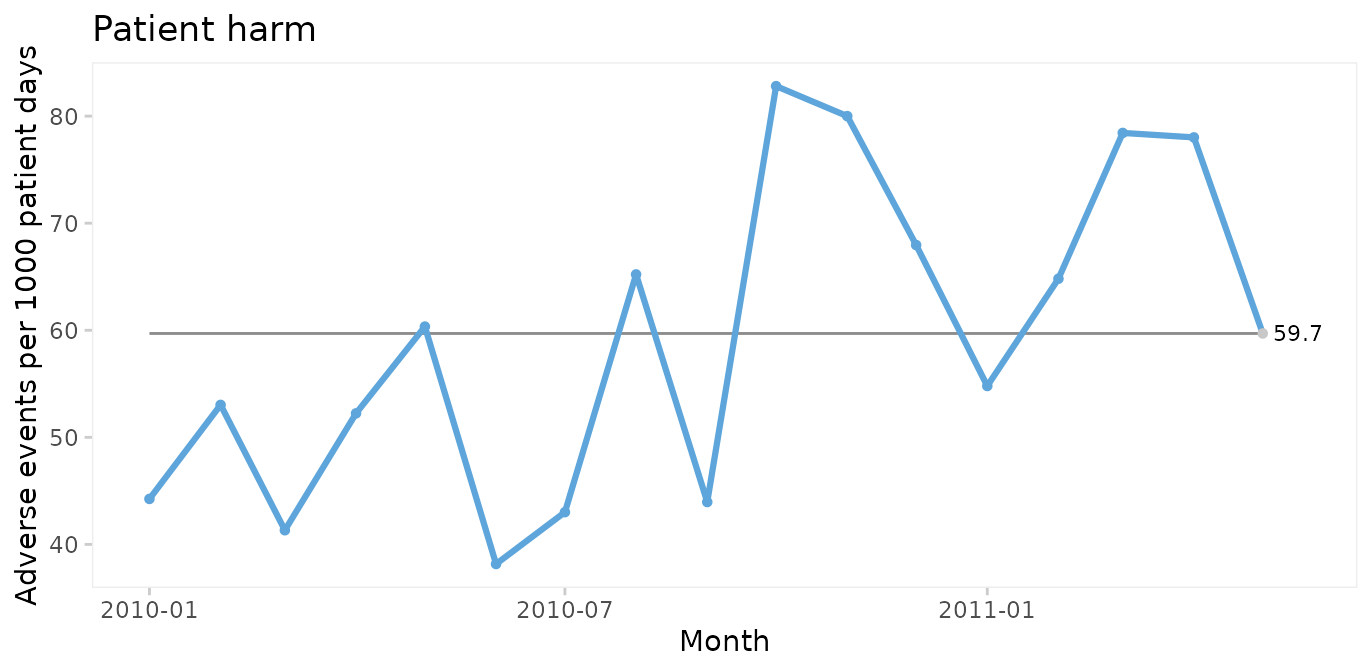
Since only random variation is present in the run chart, a U control chart for harm rate is appropriate for computing the limits of the common cause variation.
U chart of adverse events per 1000 patient days
qic(month, harms, days,
data = gtt,
chart = 'u',
multiply = 1000,
title = 'Patient harm (U chart)',
ylab = 'Adverse events per 1000 patient days',
xlab = 'Month')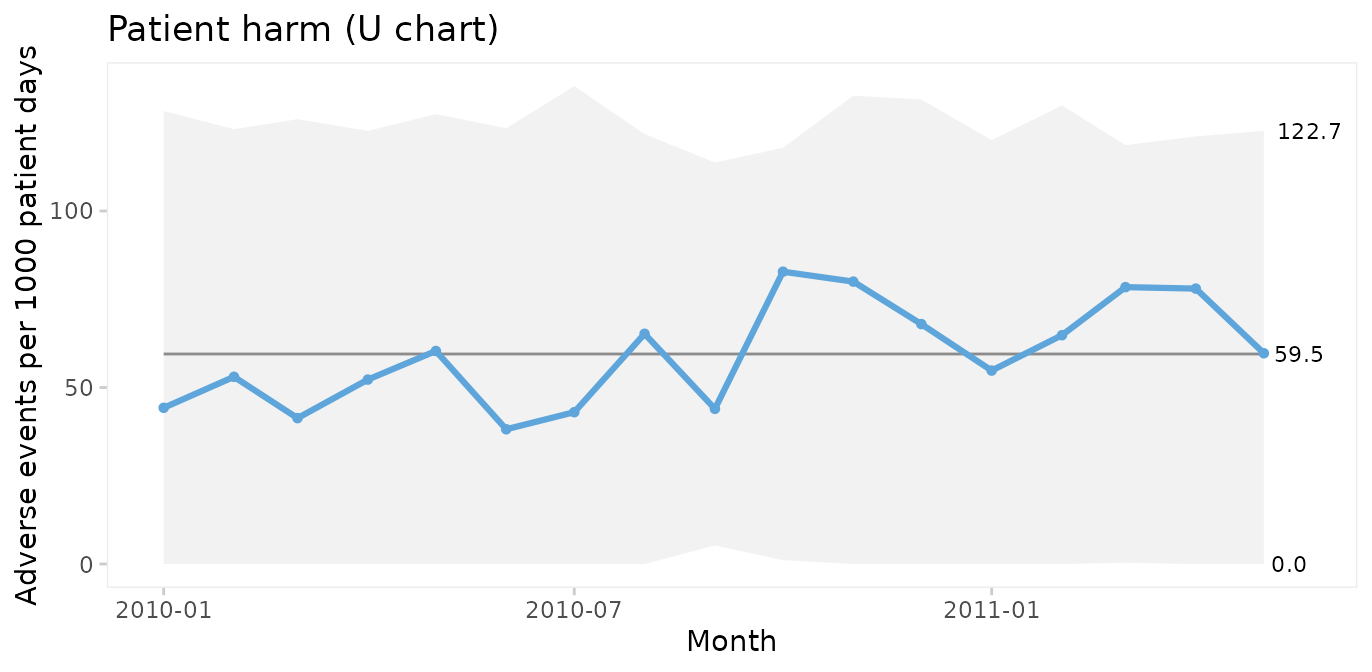
Because the sample sizes (number of patient days) are not the same each month, the 3-sigma limits vary. Large samples give narrow limits and vice versa. Varying limits are also seen in P and Xbar charts.
Run and P control charts of percent harmed patients
To plot the percentage of harmed patients (patients with 1 or more harms) we need to add a variable and to aggregate data by month.
suppressPackageStartupMessages(library(dplyr))
gtt_by_month <- gtt %>%
mutate(harmed = harms > 0) %>%
group_by(month) %>%
summarise(harms = sum(harms),
days = sum(days),
n.harmed = sum(harmed),
n = n())
head(gtt_by_month)
#> # A tibble: 6 × 5
#> month harms days n.harmed n
#> <date> <dbl> <dbl> <int> <int>
#> 1 2010-01-01 5 113 3 20
#> 2 2010-02-01 7 132 6 20
#> 3 2010-03-01 5 121 4 20
#> 4 2010-04-01 7 134 5 20
#> 5 2010-05-01 7 116 7 20
#> 6 2010-06-01 5 131 5 20
qic(month, n.harmed,
n = n,
data = gtt_by_month,
y.percent = TRUE,
title = 'Harmed patients',
ylab = NULL,
xlab = 'Month')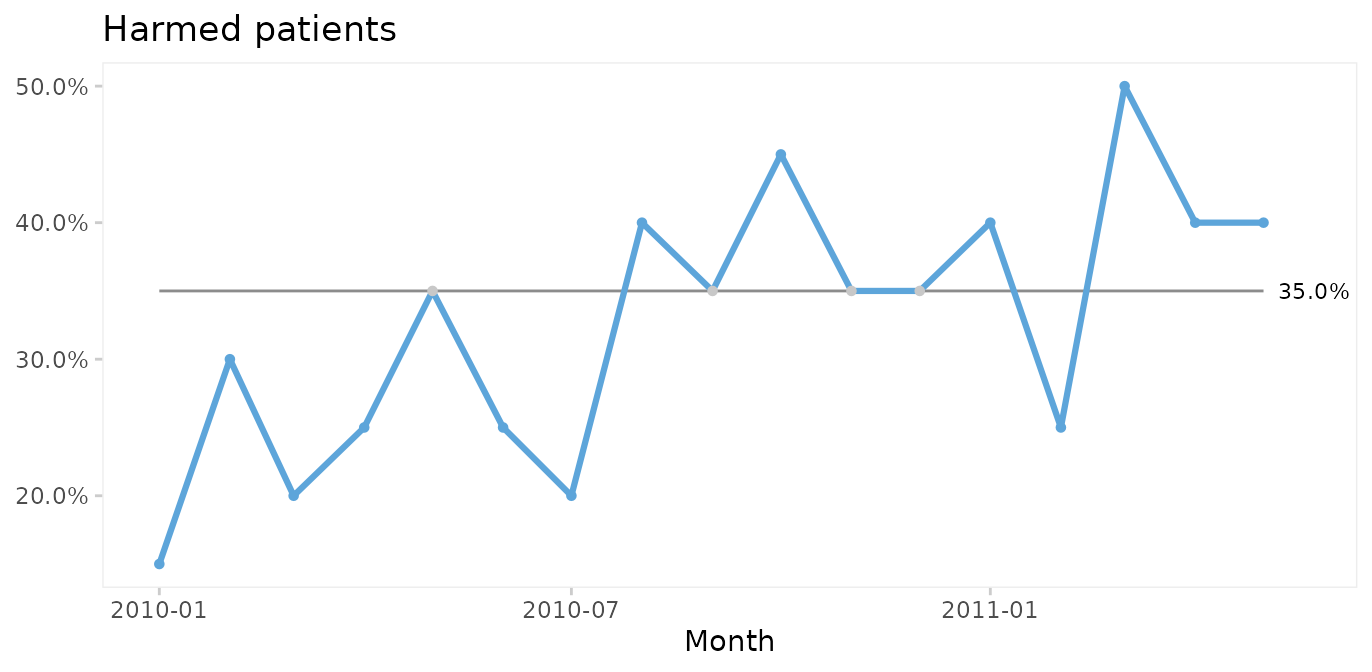
Again, since the run chart finds random variation, a control chart may be applied. For proportion (or percent) harmed patients we use a P chart.
qic(month, n.harmed, n,
data = gtt_by_month,
chart = 'p',
y.percent = TRUE,
title = 'Harmed patients (P chart)',
ylab = NULL,
xlab = 'Month')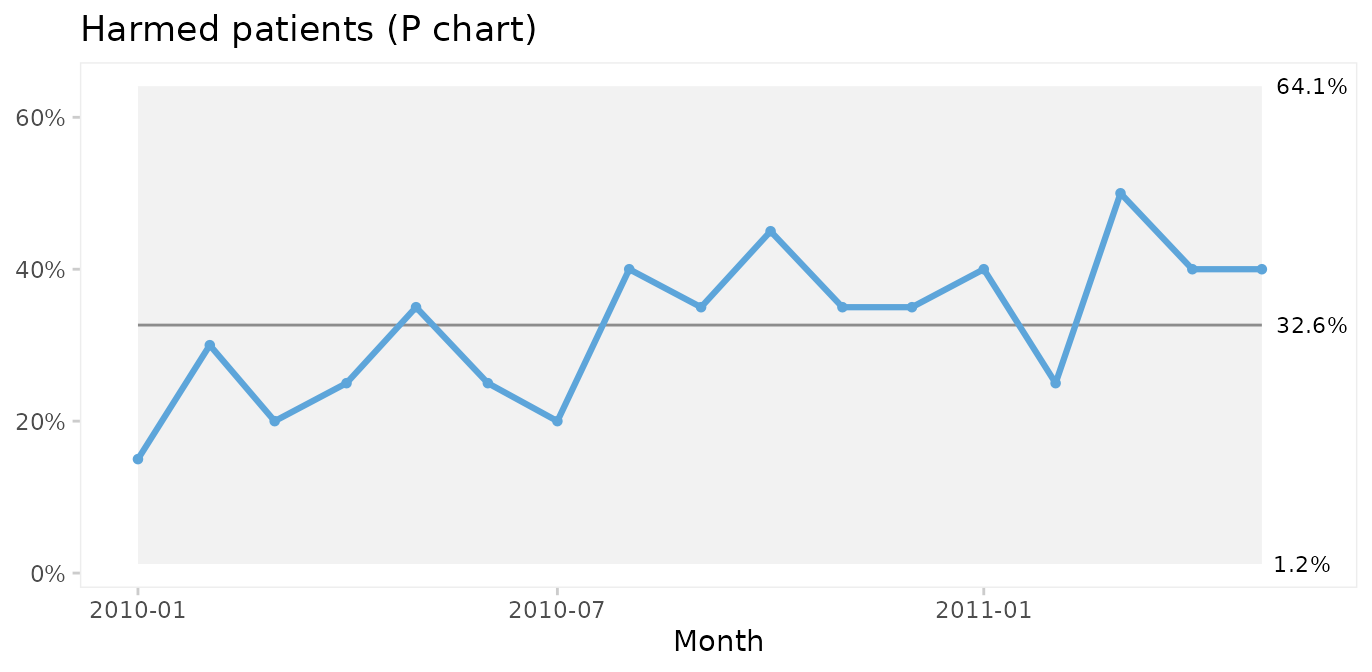
Since both the harm rate and the proportion of harmed patients exhibit common cause variation only, we conclude that the risk of adverse events during hospitalisation is predictable: we in the future should expect around 60 adverse events per 1000 patient days, harming around 33% of patients (regardless of their length of stay), although harm rates anywhere between ~0 – 60% would be considered within common cause variation.
Actually, we often do not need to aggregate data in advance. With a
little creativity we can make qic do the hard work. The
previous plot could have been produced with this code. Note the use of
the original gtt dataset and the number of harmed and total
number of patients created on the fly.
qic(month,
harms > 0, # TRUE if patient had one or more harms
days > 0, # Always TRUE
data = gtt,
chart = 'p',
y.percent = TRUE,
title = 'Harmed patients (P chart)',
ylab = NULL,
xlab = 'Month')Pareto analysis of adverse event types and severity
The Pareto chart, named after Vilfred Pareto, was invented by Joseph M. Juran as a tool to identify the most important causes of a problem.
Types and severity of adverse events in gtt are
organised in an untidy wide format. Since paretochart()
needs a vector of categorical data, we need to rearrange harm severity
and harm category into separate columns.
suppressPackageStartupMessages(library(tidyr))
gtt_ae_types <- gtt %>%
gather(severity, category, E:I) %>%
filter(complete.cases(.))
head(gtt_ae_types)
#> admission_id admission_dte discharge_dte month days harms severity
#> 1 2 2009-12-24 2010-01-06 2010-01-01 14 2 E
#> 2 11 2010-01-08 2010-01-18 2010-01-01 11 2 E
#> 3 12 2010-01-11 2010-01-19 2010-01-01 9 1 E
#> 4 29 2010-01-27 2010-02-10 2010-02-01 15 1 E
#> 5 41 2010-02-24 2010-03-01 2010-03-01 6 1 E
#> 6 45 2010-02-22 2010-03-06 2010-03-01 13 1 E
#> category
#> 1 Pressure ulcer
#> 2 Infection
#> 3 Pressure ulcer
#> 4 Pressure ulcer
#> 5 Gastrointestinal
#> 6 Gastrointestinal
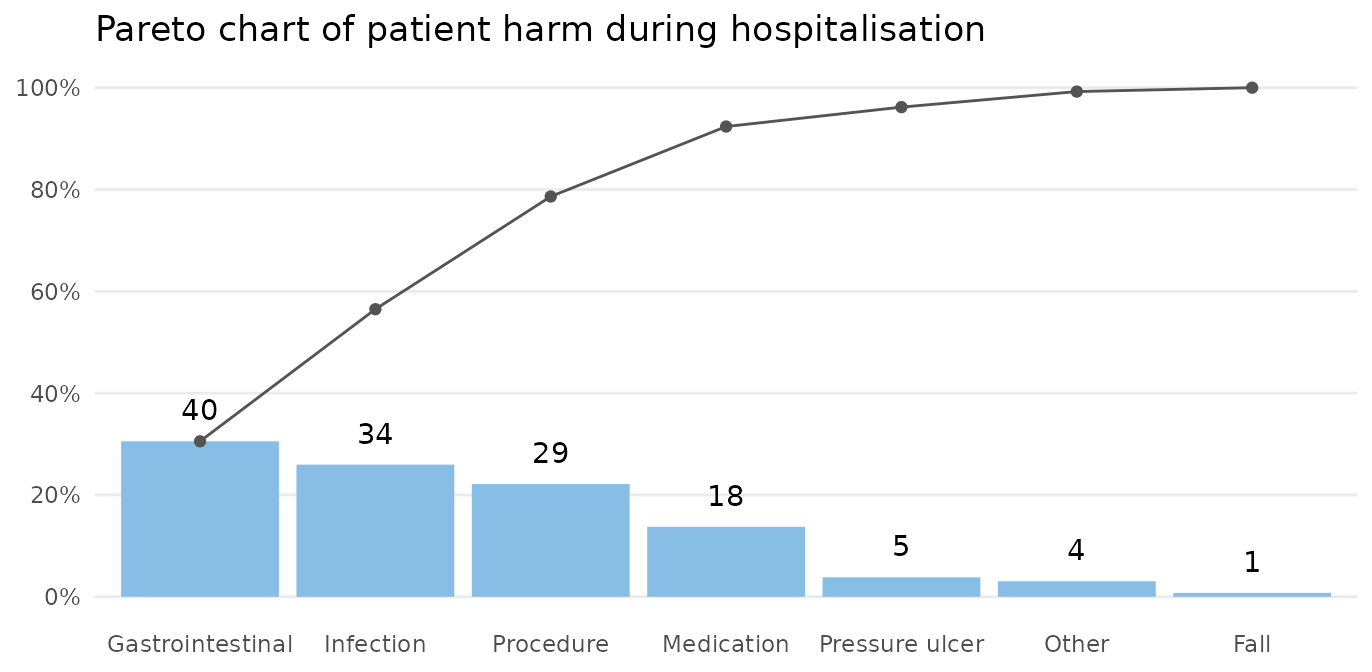
paretochart(gtt_ae_types$category,
title = 'Pareto chart of harm category')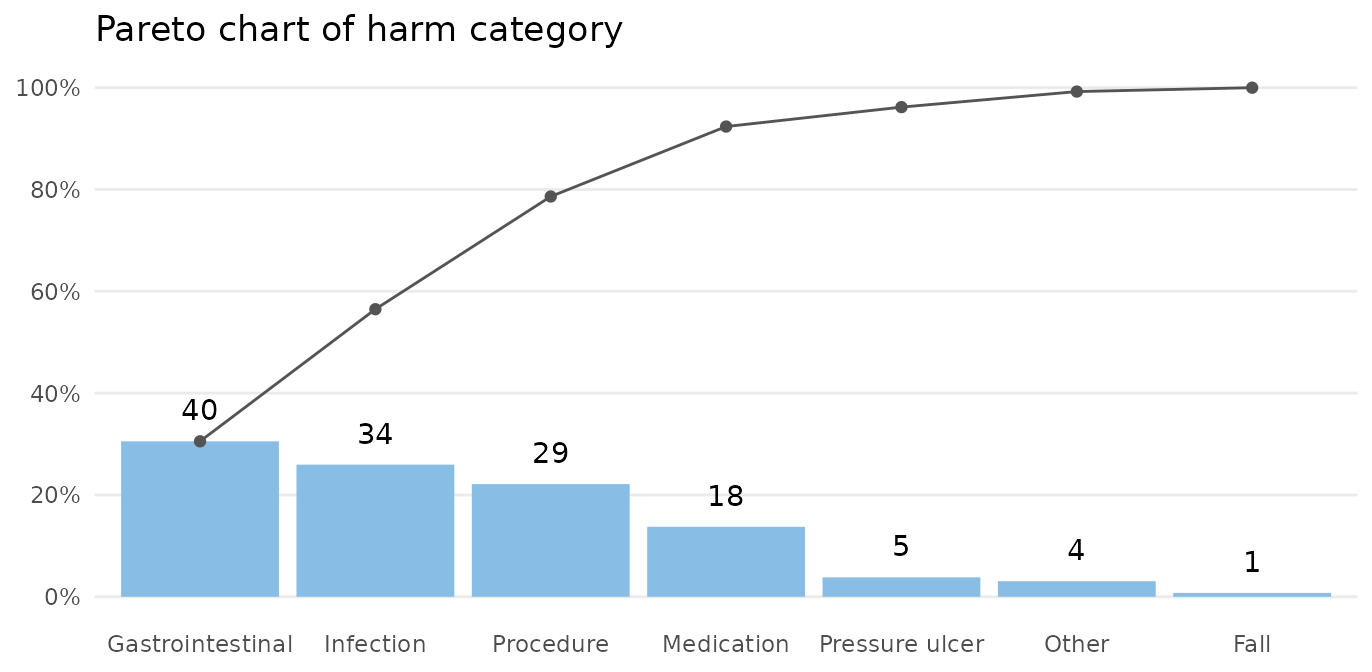
The bars show the number in each category, and the curve shows the cumulated percentage over categories. Almost 80% of harms come from 3 categories: gastrointestinal, infection, and procedure.
paretochart(gtt_ae_types$severity,
title = 'Pareto chart of harm severity')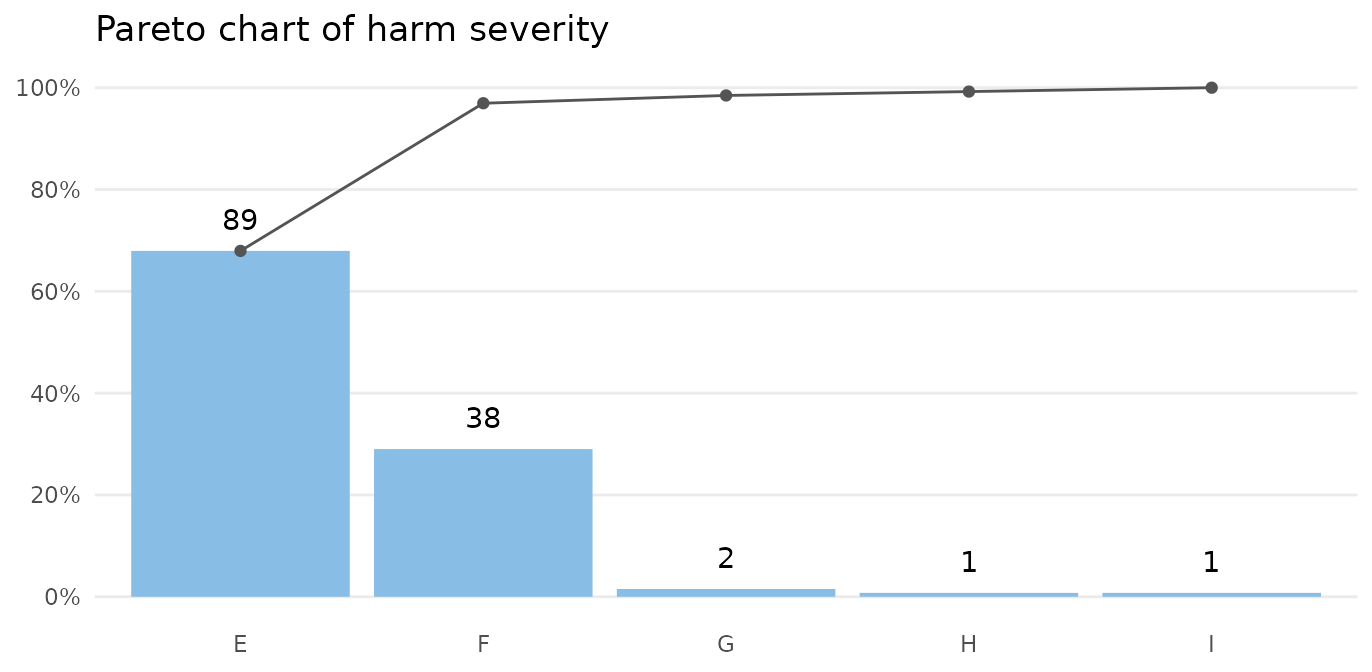
Almost all harms are temporary (E-F).
Case 2: Clostridium difficile infections
The cdi dataset contains data on hospital acquired
Clostridium difficile infections (CDI) before and after an
intervention to reduce the risk of CDI. See ?cdi for
details.
head(cdi)
#> month n days period notes
#> 1 2012-11-01 17 14768.42 pre <NA>
#> 2 2012-12-01 12 14460.33 pre <NA>
#> 3 2013-01-01 27 16176.92 pre <NA>
#> 4 2013-02-01 20 14226.50 pre <NA>
#> 5 2013-03-01 20 14816.25 pre <NA>
#> 6 2013-04-01 18 14335.29 pre <NA>Run charts for number of infections
We begin by plotting a run chart of the number of CDIs per month.
qic(month, n,
notes = notes,
data = cdi,
decimals = 0,
title = 'Hospital acquired Clostridium difficile infections',
ylab = 'Count',
xlab = 'Month')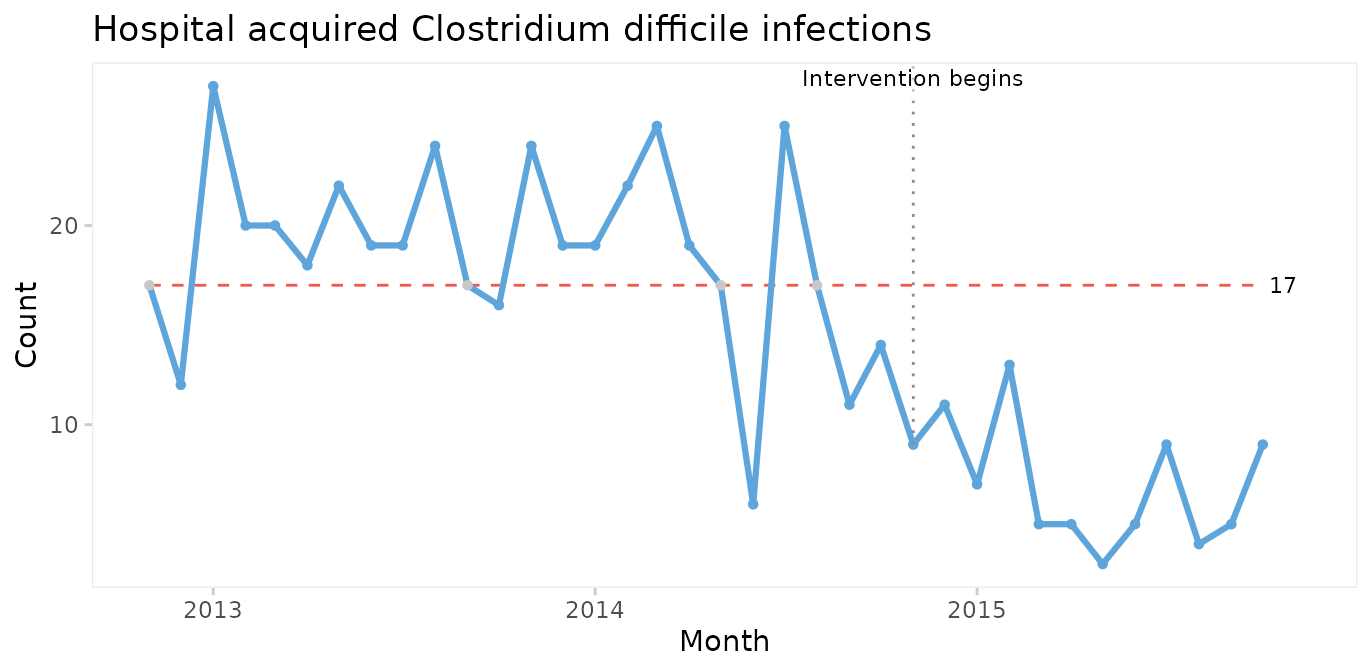
A downward shift in the number of CDIs is clearly visible to the naked eye and is supported by the runs analysis resulting in the centre line being dashed red. The shift seem to begin around the time of the intervention.
Even though it is not necessary in this case, we can strengthen the analysis by using the median of the before-intervention period to test for non-random variation in the after period.
qic(month, n,
data = cdi,
decimals = 0,
freeze = 24,
part.labels = c('Baseline', 'Intervention'),
title = 'Hospital acquired Clostridium difficile infections',
ylab = 'Count',
xlab = 'Month')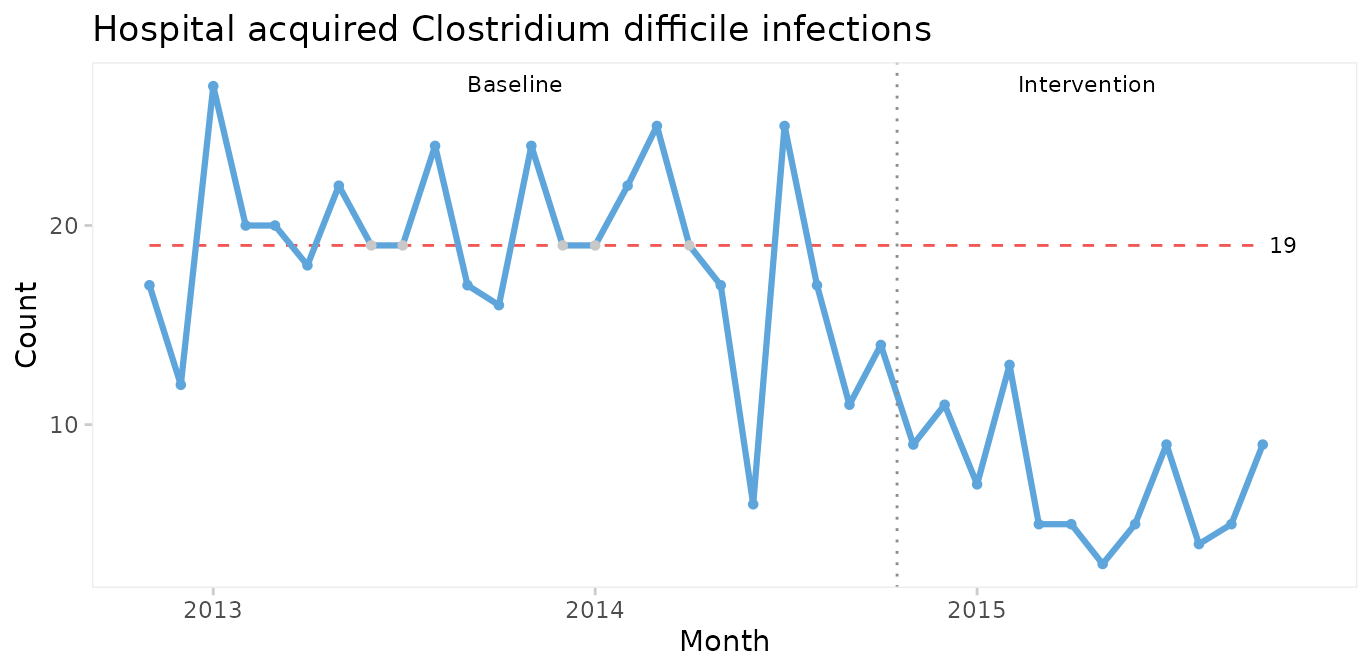
The median number of CDIs per month in the before period is 19. An unusually long run of 15 data points below the median proves that the CDI rate is reduced.
When a shift in the desired direction is the result of a deliberate change to the process, we may split the chart to compare the numbers before and after the intervention.
qic(month, n,
data = cdi,
decimals = 0,
part = 24,
title = 'Hospital acquired Clostridium difficile infections',
ylab = 'Count',
xlab = 'Month')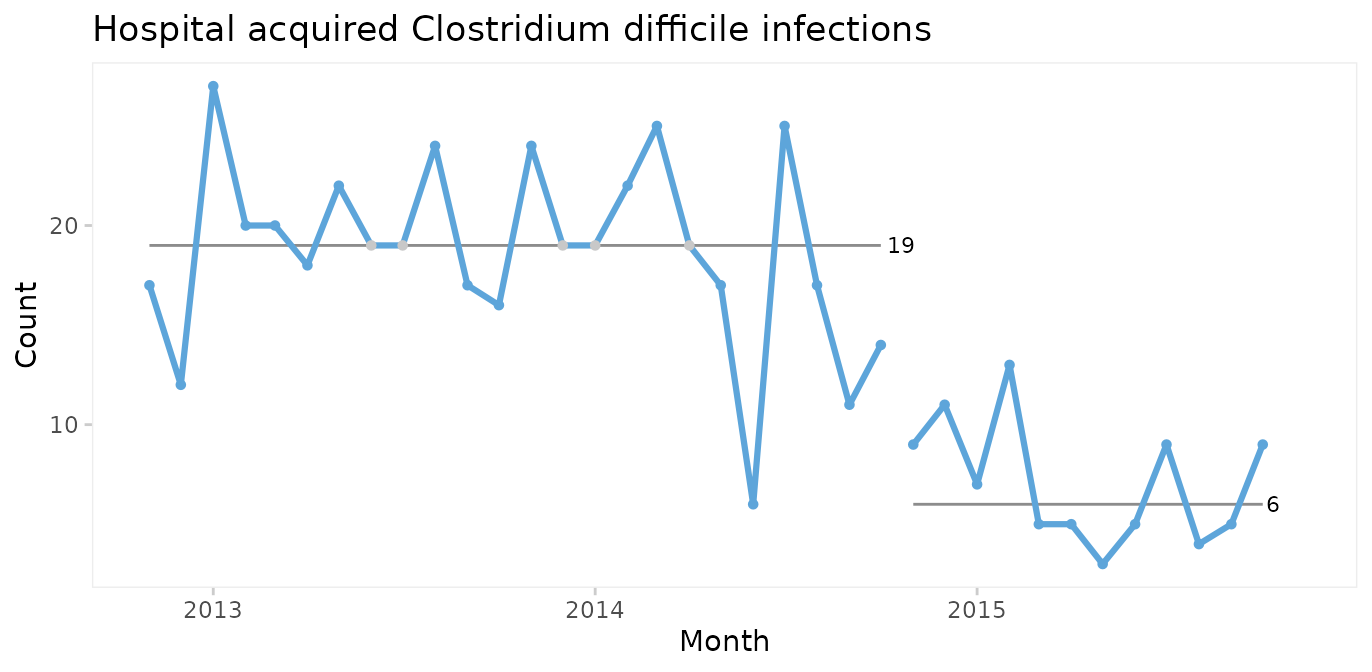
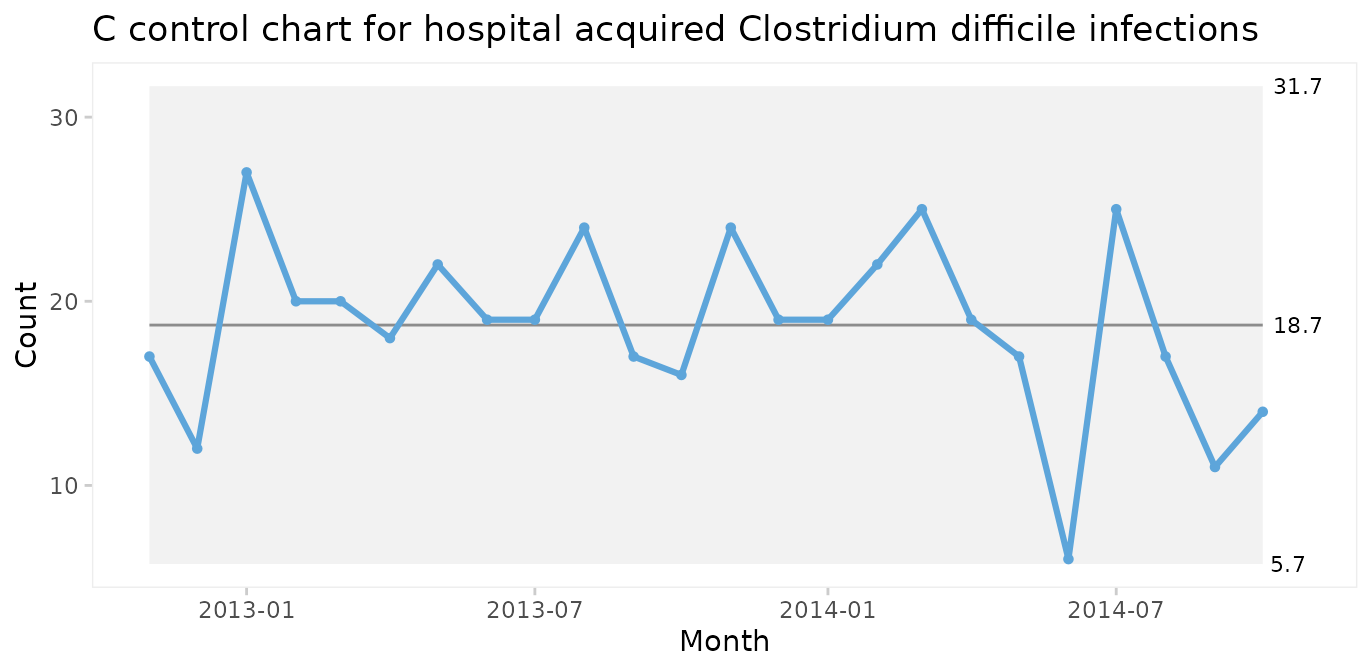
C chart for number of infections
Since both periods show only random variation, a control chart may be applied to test for larger transient shifts in data and to establish the natural limits of the current process. The correct chart in this case is the C chart for number of infections.
qic(month, n,
data = cdi,
chart = 'c',
part = 24,
title = 'Hospital acquired Clostridium difficile infections (C chart)',
ylab = 'Count',
xlab = 'Month')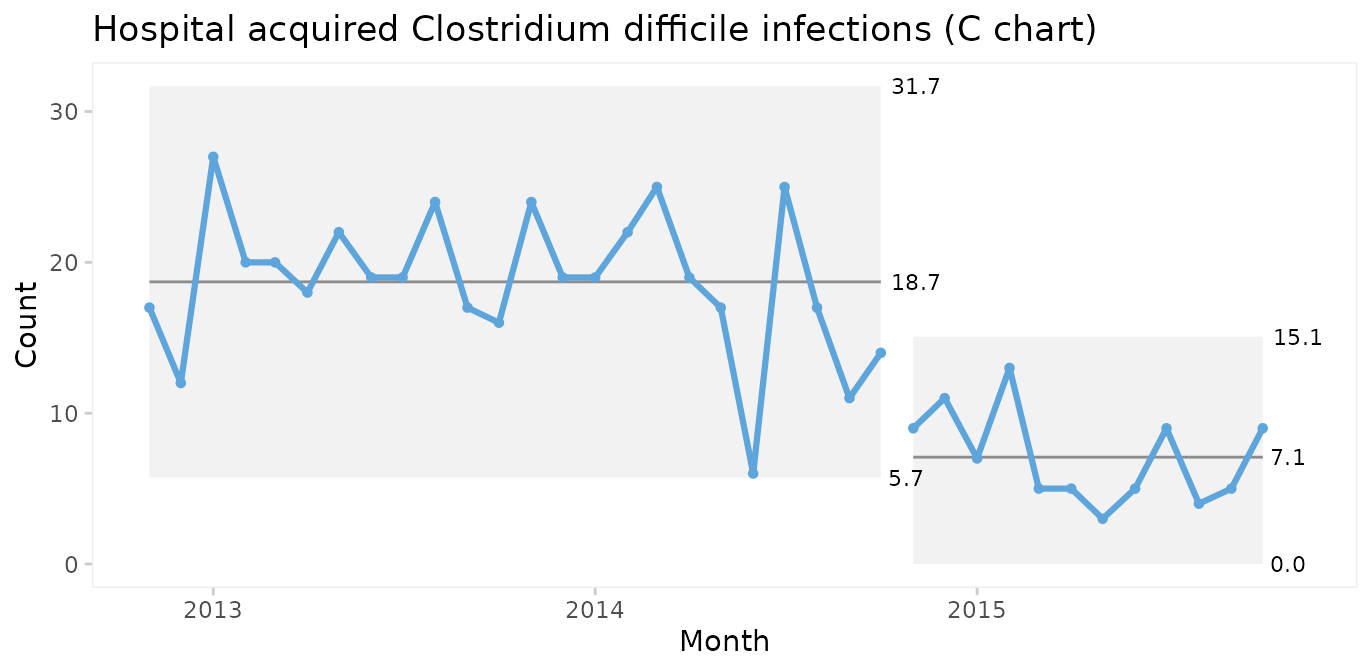
The split C chart shows that the CDI rate has dropped from an average of 19 to 7 per month. Furthermore, the 3-sigma limits tell that the current process is predictable and that we in the future should expect between 0 and 15 CDIs per month.
U chart for infection rate
Until now we have assumed that the area of opportunity, or exposure, is constant, i.e., the number of patients or patient days have not changed significantly over time. When the area of opportunity varies, a U chart (U for unequal area of opportunity) is more appropriate.
qic(month, n, days,
data = cdi,
chart = 'u',
part = 24,
multiply = 10000,
title = 'Hospital acquired Clostridium difficile infections (U chart)',
ylab = 'Cases per 10,000 risk days',
xlab = 'Month')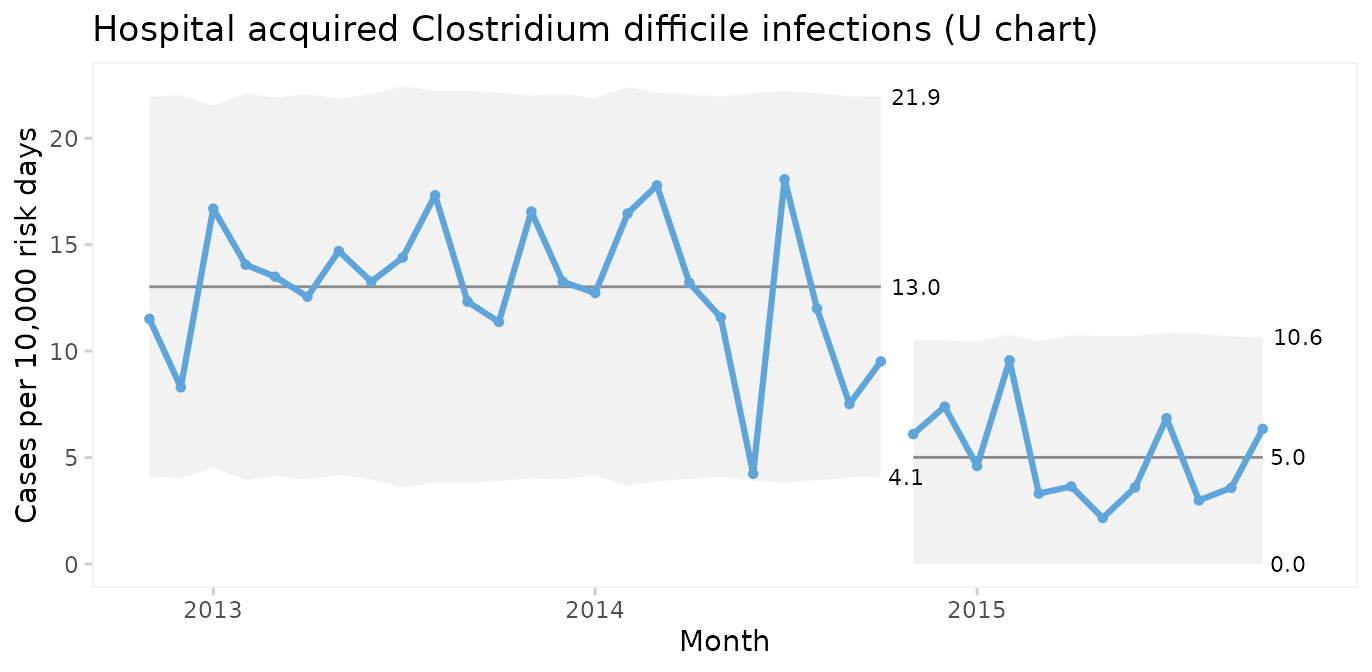
In fact, U charts can always be used instead of C charts. When the area of opportunity is constant the two charts will reach the same conclusion. But the raw numbers in a C chart may be easier to communicate than counts per something.
It is very important to recognise that while run and control charts can identify non-random variation, they cannot identify its causes. The analysis only tells that the CDI rate was reduced after an intervention. The causal relationship between the intervention and the shift must be established using other methods.
When should you recompute the limits?
When splitting a chart as in the example above you make a deliberate decision based on your understanding of the process. Some software packages offer automated recalculation of limits whenever a shift is detected. I find this approach very wrong. Limits are the voice of the process and recomputing limits without understanding the context, which computers don’t, is like telling someone to shut up, when they are really trying to tell you something important.
Wheeler suggests that limits may be recomputed when the answers to all four of these question is “yes” (Wheeler 2010, p. 224):
Do the data display a distinctly different kind of behaviour than in the past?
Is the reason for this change in behaviour known?
Is the new process behaviour desirable?
Is it intended and expected that the new behaviour will continue?
If the answer to any of these question is “no”, you should rather seek to find the assignable cause of the shift and, if need be, eliminate it.
Thus, when a deliberate change has been made to the process and the chart finds a shift attributable to this change, it may be time to recompute the limits.
Case 3: Coronary artery bypass graft
The cabg dataset contains data on individual coronary
artery bypass operations. See ?cabg for details.
head(cabg)
#> date age gender los death readmission
#> 1 2011-07-01 72.534 Male 8 FALSE TRUE
#> 2 2011-07-01 59.225 Male 9 FALSE FALSE
#> 3 2011-07-04 66.841 Male 15 FALSE FALSE
#> 4 2011-07-04 70.337 Male 9 FALSE FALSE
#> 5 2011-07-04 60.816 Male 6 FALSE TRUE
#> 6 2011-07-05 57.027 Male 9 FALSE FALSEI and MR charts for age of individual patients
In this and the following cases we skip the obligatory first step of using a run chart.
First, we will make a control chart of the age of the last 100 patients. Since we are plotting individual measurements, we use an I chart.
qic(age,
data = tail(cabg, 100),
chart = 'i',
show.grid = TRUE,
title = 'Age of the last 100 patients (I chart)',
ylab = 'Years',
xlab = 'Patient #')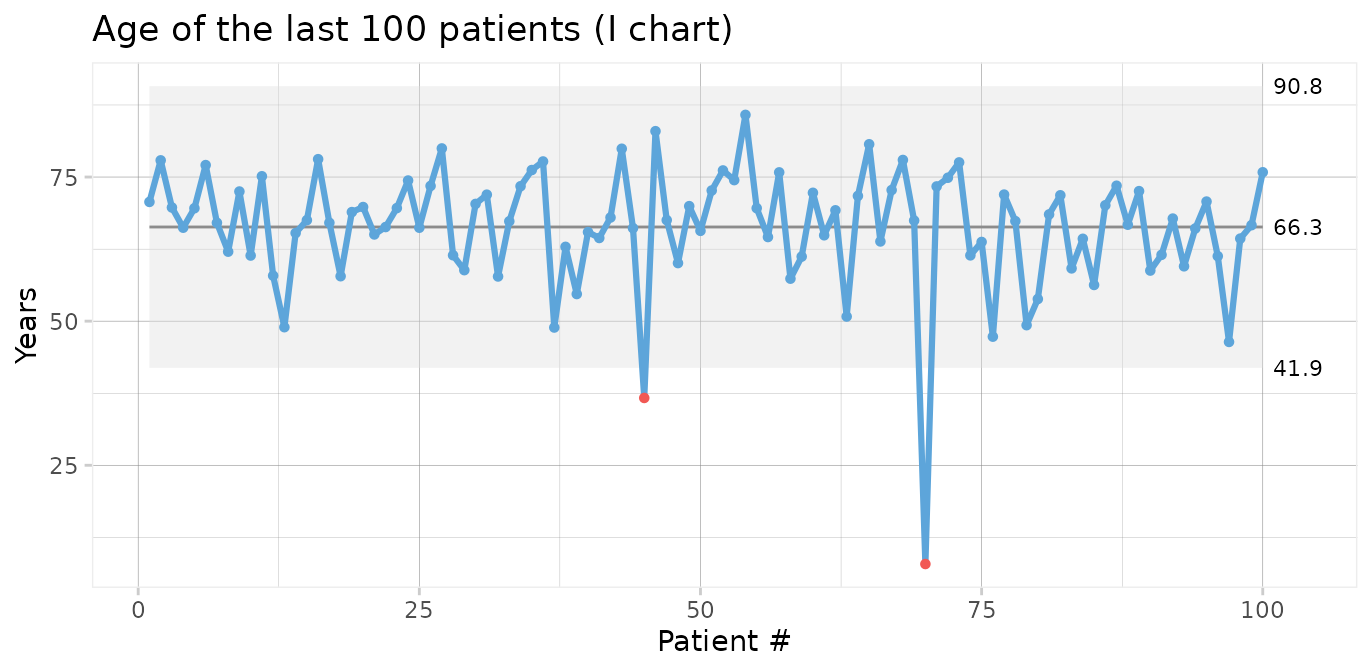
Two data points (patients number 45 and 70) are below the lower 3-sigma limit indicating that these patients are “unusually” young, i.e. representative of phenomena that are not normally present in the process.
I charts are often displayed along moving range charts that show the ranges of neighbouring data points.
qic(age,
data = tail(cabg, 100),
chart = 'mr',
show.grid = TRUE,
title = 'Age of the last 100 patients (MR chart)',
ylab = 'Years',
xlab = 'Patient #')
The MR chart identifies three unusually large ranges, which are clearly produced by the two unusually young patients also found in the I chart. Note that each data point in an I chart is contained in two moving ranges in the MR chart.
We should seek the cause(s) of these special causes. We may then chose to eliminate the outliers from the computations of the process centre and 3-sigma limits in order to predict the expected age range of future patients.
qic(age,
data = tail(cabg, 100),
chart = 'i',
exclude = c(45, 70),
title = 'Age of the last 100 patients (I chart)',
ylab = 'Years',
xlab = 'Patient #')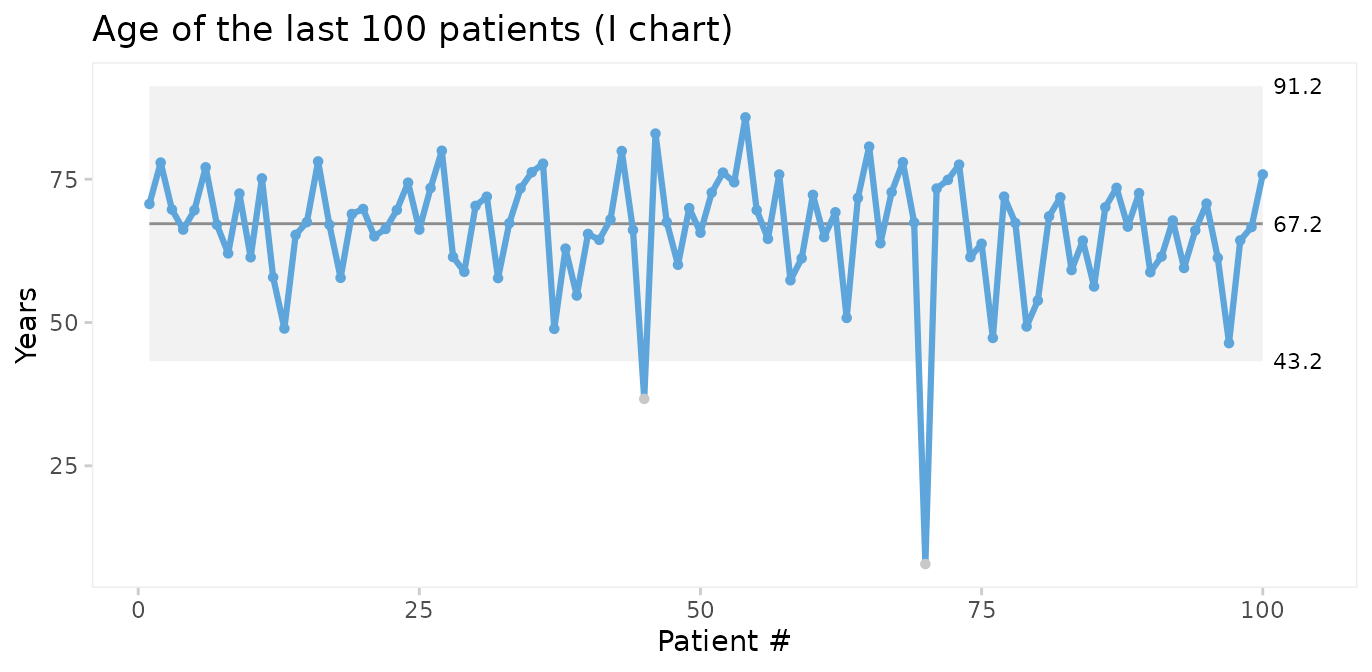
Thus, on average we should expect future patients to be 67 years of age, and patients younger than 43 years or older than 91 years would be unusual.
Xbar and S charts for average and standard deviation of patient age
We could also plot the mean age of patients by month. For this we choose an Xbar chart for multiple measurement per subgroup. First, we need to add month as the grouping variable.
Using month as the x axis variable, qic() automatically
calculates the average age per month.
qic(month, age,
data = cabg,
chart = 'xbar',
title = 'Average age (Xbar chart)',
ylab = 'Years',
xlab = 'Month')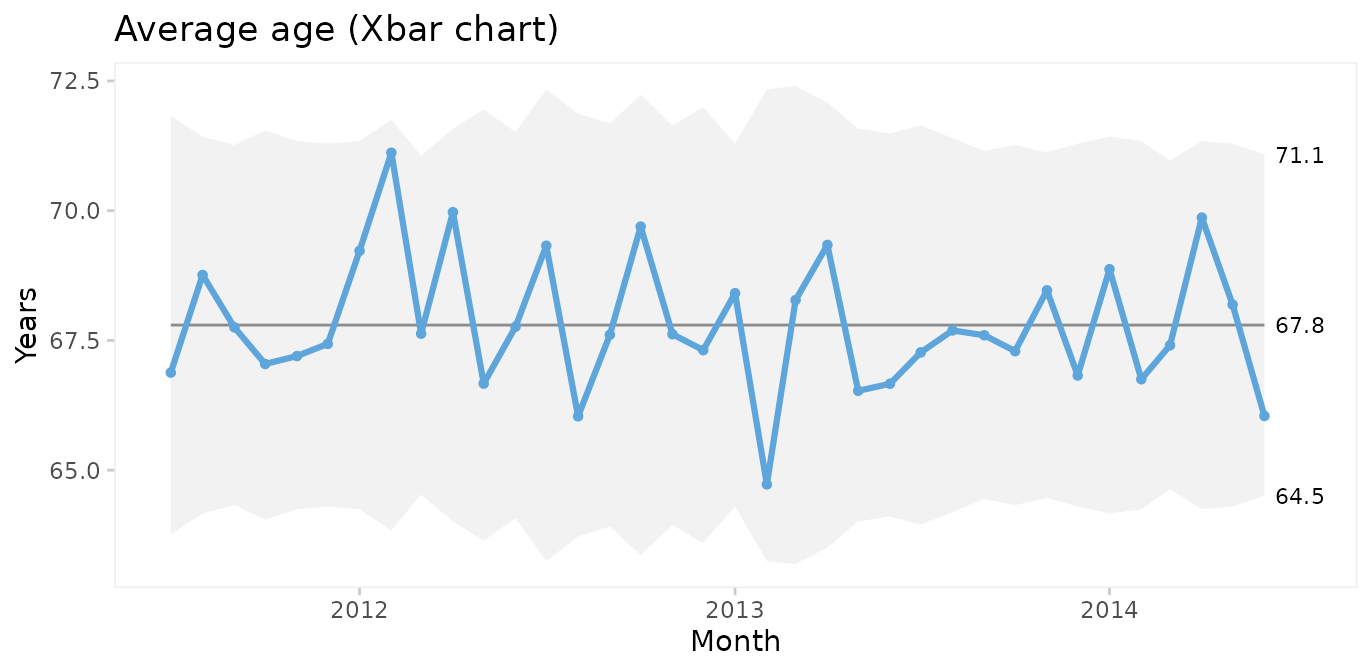
Xbar charts are usually displayed along S charts displaying the within subgroup standard deviation.
qic(month, age,
data = cabg,
chart = 's',
title = 'Age standard deviation (S chart)',
ylab = 'Years',
xlab = 'Month')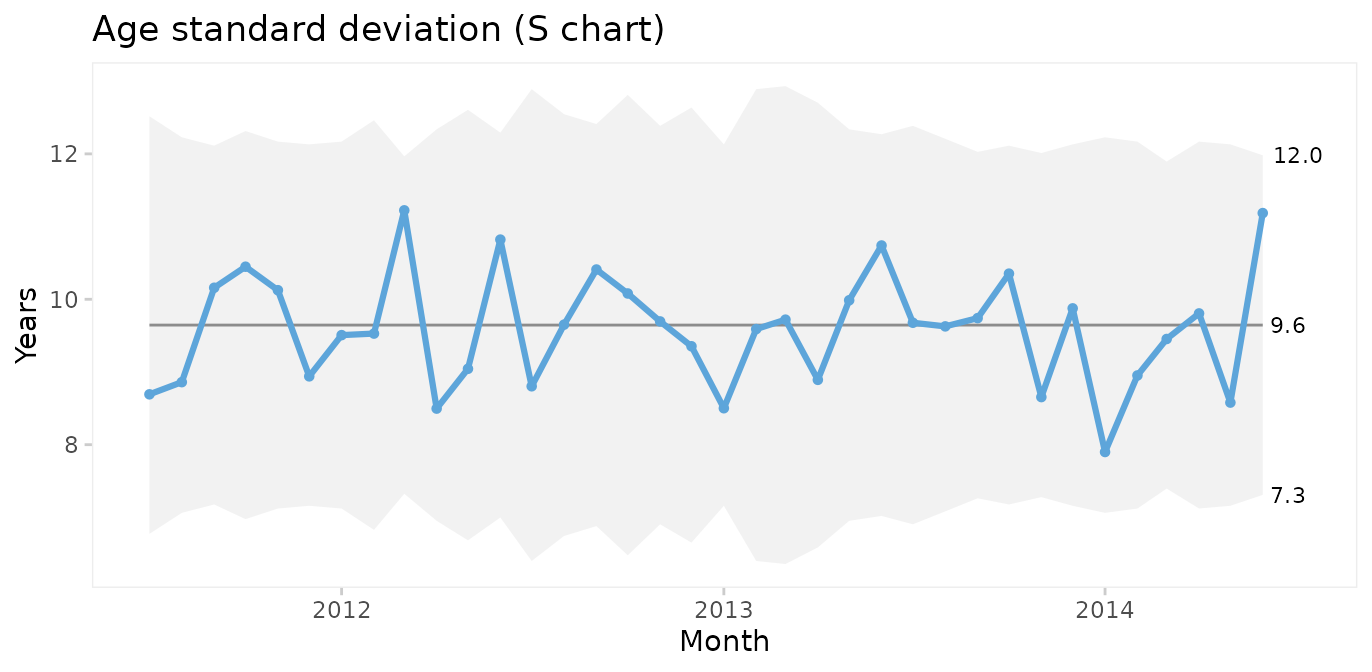
Since both the Xbar and the S chart display common cause variation, we may conclude that the monthly average and standard deviation of patient age is predictable. Note that the mean of the Xbar chart is close to the mean of the individuals chart but that the 3-sigma limits are narrower.
P charts for proportion of patients who were readmitted or died within 30 after surgery
To plot readmissions and mortality we first need to summarise these counts by month.
cabg_by_month <- cabg %>%
group_by(month) %>%
summarise(deaths = sum(death),
readmissions = sum(readmission),
n = n())
head(cabg_by_month)
#> # A tibble: 6 × 4
#> month deaths readmissions n
#> <date> <int> <int> <int>
#> 1 2011-07-01 1 14 52
#> 2 2011-08-01 3 12 64
#> 3 2011-09-01 2 15 70
#> 4 2011-10-01 1 8 60
#> 5 2011-11-01 1 16 67
#> 6 2011-12-01 3 11 69Then we use P charts for proportion of readmissions.
qic(month, readmissions, n,
data = cabg_by_month,
chart = 'p',
y.percent = TRUE,
title = 'Readmissions within 30 days (P chart)',
ylab = NULL,
xlab = 'Month')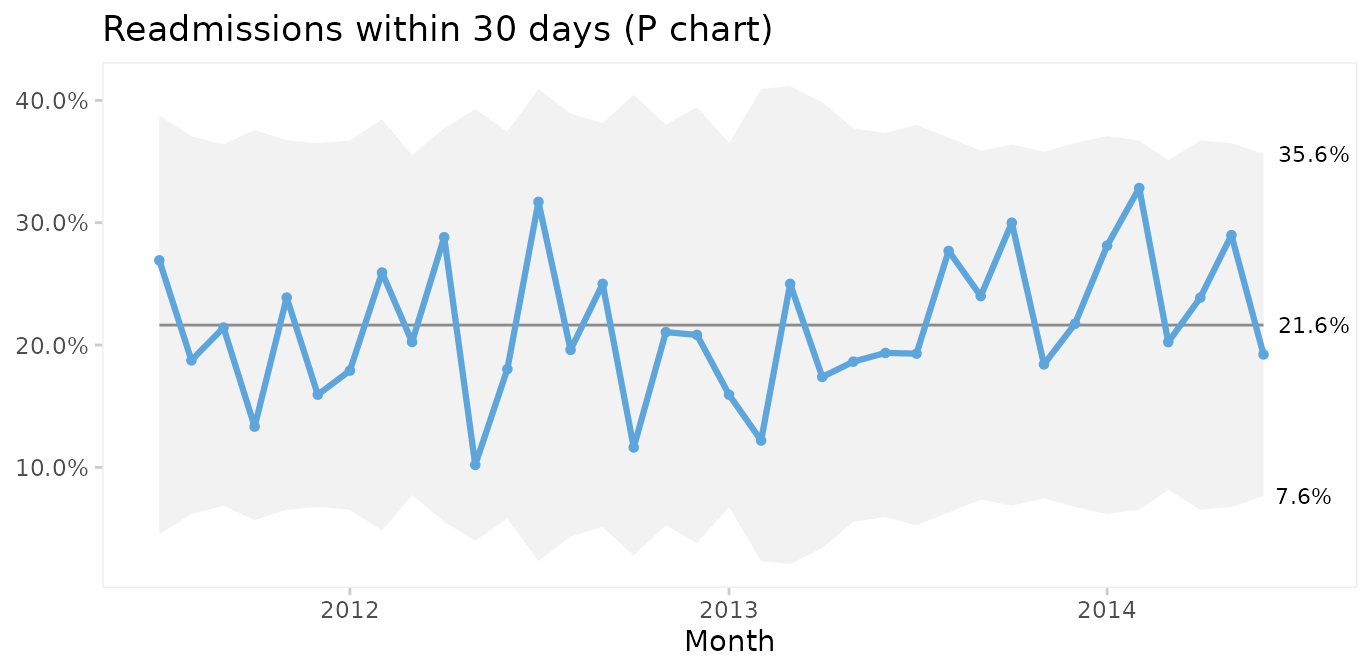
On average, 22% of patients are readmitted within 30 days after surgery, and if nothing changes we would expect this to continue.
What about mortality?
qic(month, deaths, n,
data = cabg_by_month,
chart = 'p',
y.percent = TRUE,
title = '30 days mortality (P chart)',
ylab = NULL,
xlab = 'Month')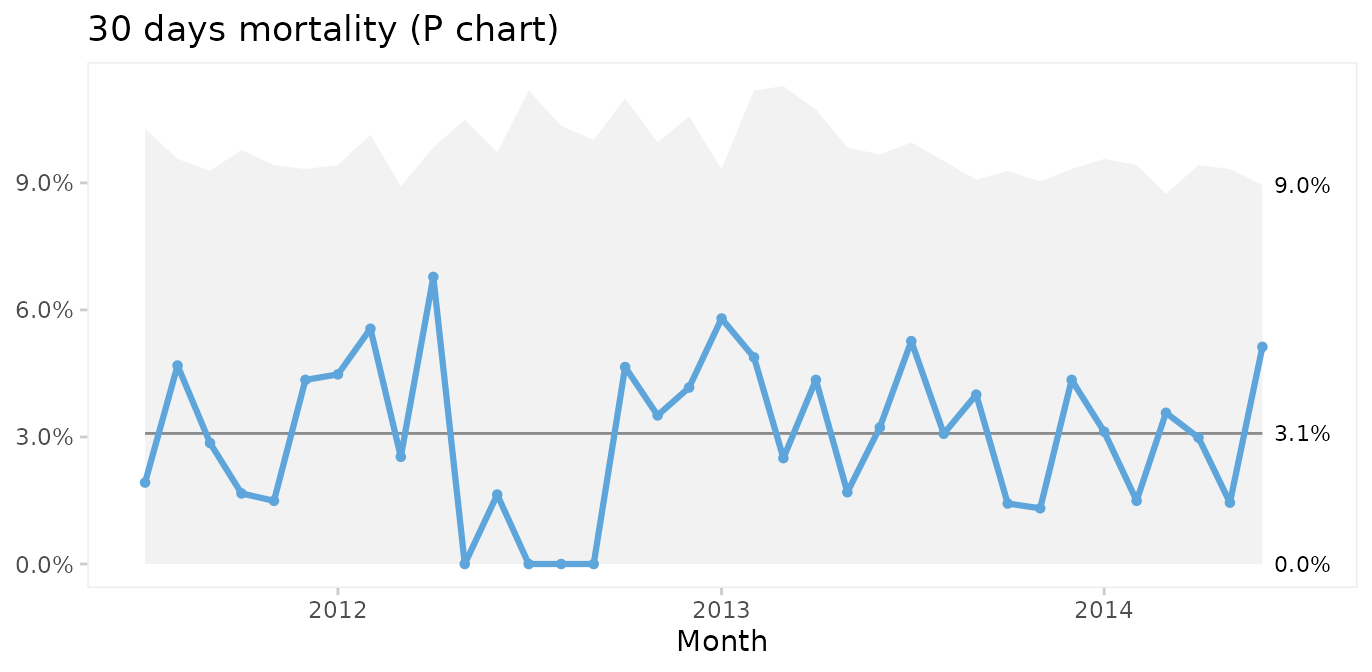
Thankfully, post-surgery mortality is a rare event, and the P chart suggests common cause variation. However, it seems curious that only one patient died during the summer of 2012. To investigate this further, G or T charts for rare events are useful.
T and G charts for rare events
Rare events are often better analysed as time or opportunities between events. First, we need to calculate the number of surgeries and days between fatalities.
fatalities <- cabg %>%
mutate(x = row_number()) %>%
filter(death) %>%
mutate(dd = x - lag(x) - 1, # subtract 1 to get number between
dt = date - lag(date))
head(fatalities)
#> date age gender los death readmission month x dd dt
#> 1 2011-07-21 91.227 Female 5 TRUE FALSE 2011-07-01 37 NA NA days
#> 2 2011-08-06 71.773 Male 2 TRUE FALSE 2011-08-01 60 22 16 days
#> 3 2011-08-26 73.942 Male 1 TRUE FALSE 2011-08-01 99 38 20 days
#> 4 2011-08-31 80.293 Male 3 TRUE FALSE 2011-08-01 114 14 5 days
#> 5 2011-09-13 75.359 Male 12 TRUE FALSE 2011-09-01 148 33 13 days
#> 6 2011-09-14 72.019 Female 19 TRUE FALSE 2011-09-01 149 0 1 daysThen we use a G chart for opportunities (surgeries) between events (deaths).
qic(dd,
data = fatalities,
chart = 'g',
title = 'Surgeries between deaths (G chart)',
ylab = 'Count',
xlab = 'Death #')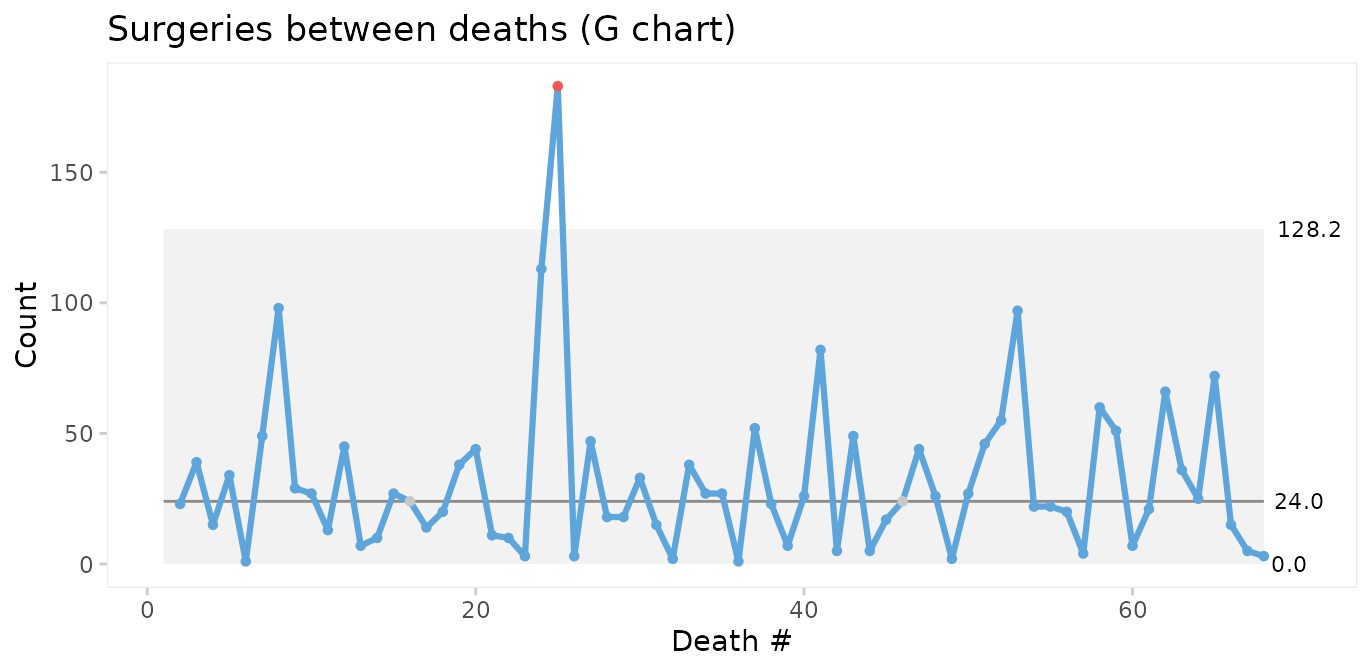
If we do not have information on the opportunities (surgeries with survival), we may instead use a T chart for time between events.
qic(dt,
data = fatalities,
chart = 't',
title = 'Days between deaths (T chart)',
ylab = 'Days',
xlab = 'Death #')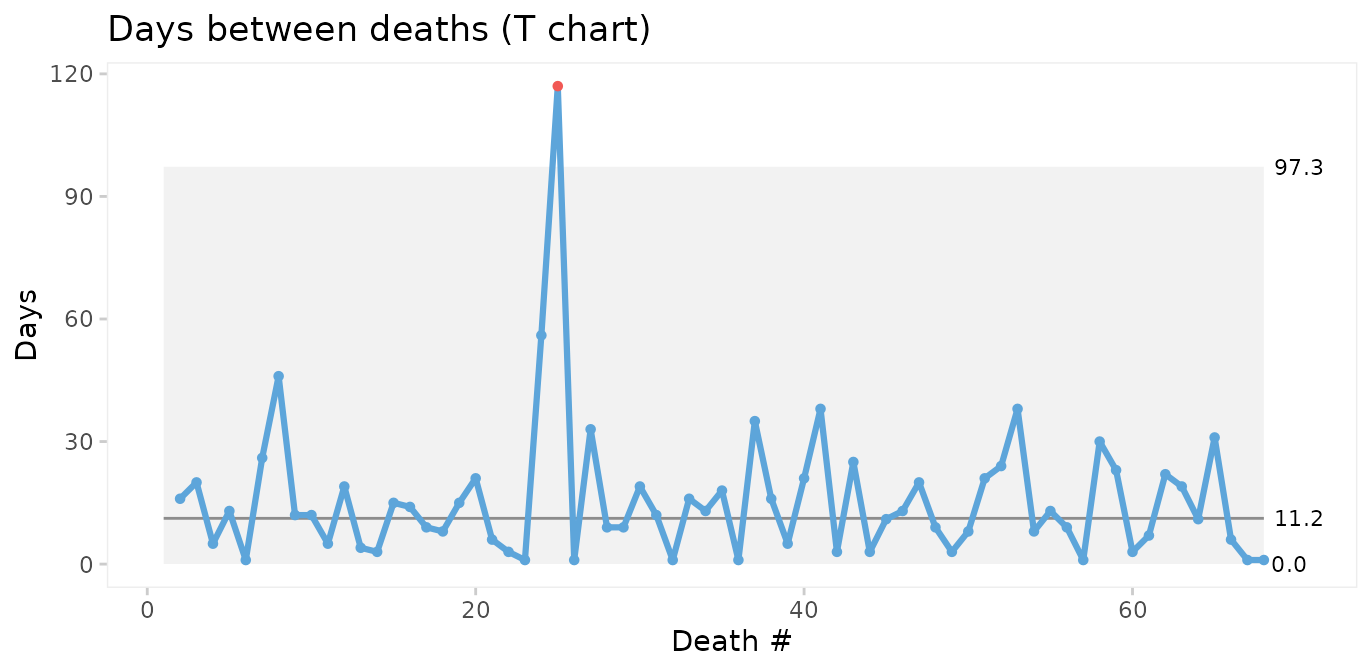
The conclusions from the two charts are the same: Deaths number 24 and 25 are unusually far apart. We should look for an assignable cause to explain this as it may help us get ideas to reduce postoperative mortality in the future.
Faceting readmission rates by gender
To demonstrate the use of faceted charts, we summarise readmissions by month and gender.
cabg_by_month_gender <- cabg %>%
group_by(month, gender) %>%
summarise(readmissions = sum(readmission),
n = n())
#> `summarise()` has regrouped the output.
#> ℹ Summaries were computed grouped by month and gender.
#> ℹ Output is grouped by month.
#> ℹ Use `summarise(.groups = "drop_last")` to silence this message.
#> ℹ Use `summarise(.by = c(month, gender))` for per-operation grouping
#> (`?dplyr::dplyr_by`) instead.
head(cabg_by_month_gender)
#> # A tibble: 6 × 4
#> # Groups: month [3]
#> month gender readmissions n
#> <date> <fct> <int> <int>
#> 1 2011-07-01 Female 2 9
#> 2 2011-07-01 Male 12 43
#> 3 2011-08-01 Female 0 9
#> 4 2011-08-01 Male 12 55
#> 5 2011-09-01 Female 3 18
#> 6 2011-09-01 Male 12 52Then we use the facets argument to make a control chart
for each gender while keeping the x and y axes the same.
qic(month, readmissions, n,
data = cabg_by_month_gender,
facets = ~ gender,
chart = 'p',
y.percent = TRUE,
title = 'Readmissions within 30 days (P chart)',
ylab = '',
xlab = 'Month')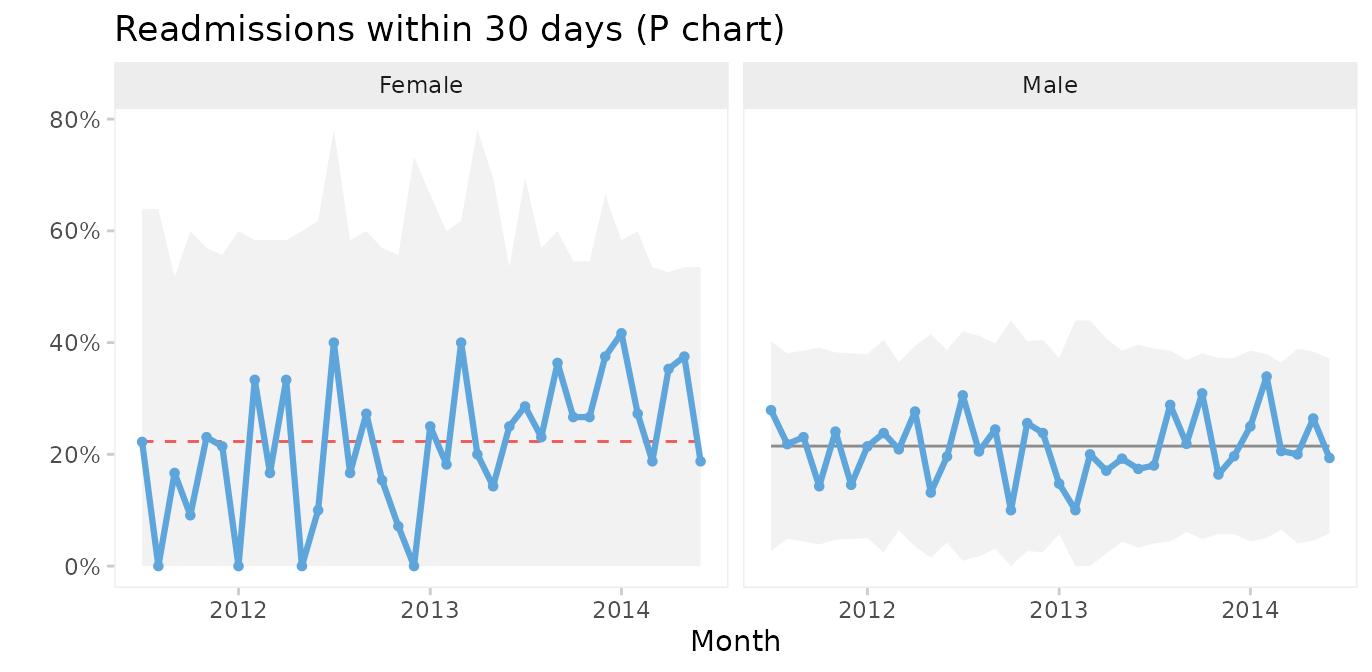
This chart suggests that the readmission rate for females is increasing. This is clearly undesirable and we should investigate this to find and eliminate the special cause.
Case 4: Faceting hospital infections by hospital and infection
The hospital_infection dataset contains data on hospital
acquired bacteremias (BAC), Clostridium difficile infections
(CDI), and urinary tract infections (UTI) from six hospitals in the
Capital Region of Denmark. See ?hospital_infections for
details.
head(hospital_infections)
#> hospital infection month n days
#> 1 AHH BAC 2015-01-01 17 17233.67
#> 2 AHH BAC 2015-02-01 18 15308.25
#> 3 AHH BAC 2015-03-01 17 16883.67
#> 4 AHH BAC 2015-04-01 10 15463.83
#> 5 AHH BAC 2015-05-01 13 15788.96
#> 6 AHH BAC 2015-06-01 14 15660.04U chart of the total number of infections per 10,000 risk days
qic(month, n, days,
data = hospital_infections,
chart = 'u',
multiply = 10000,
title = 'Hospital acquired infections in the Capital Region of Denmark',
ylab = 'Cases per 10,000 risk days',
xlab = 'Month')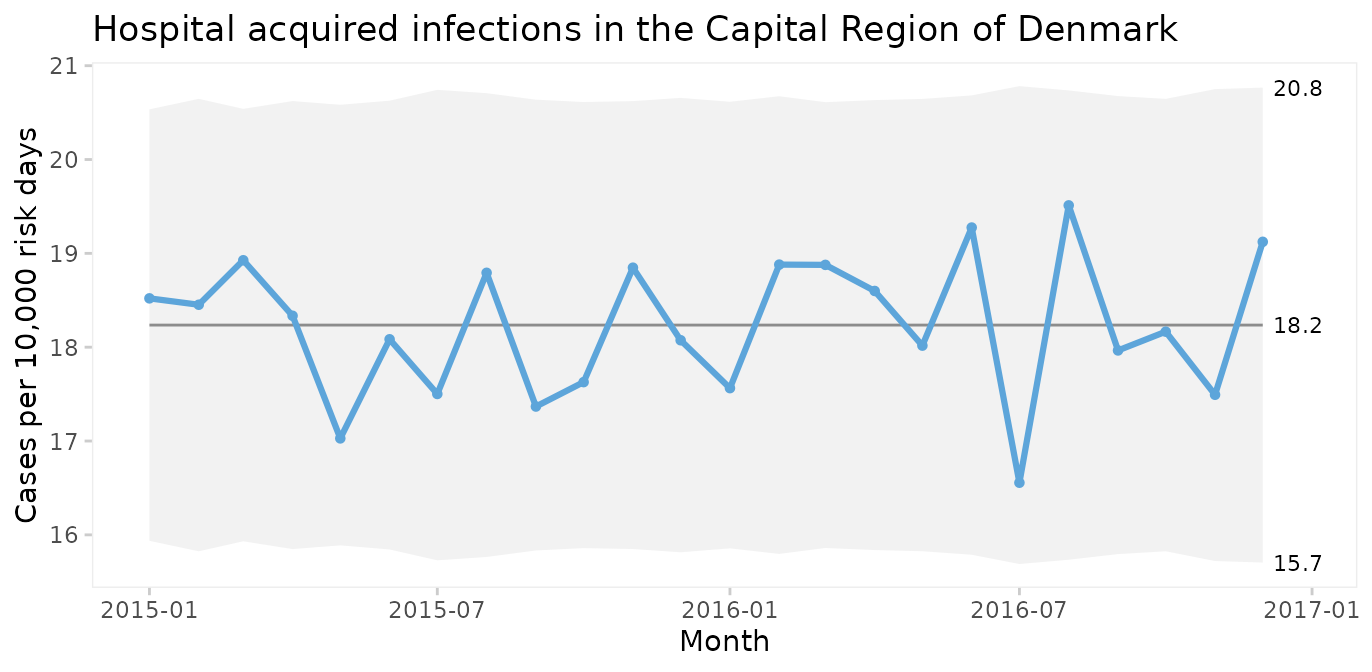
The infection rate appears predictable. However, plotting three types of infection together is like mixing apples and oranges.
Faceted U chart by type of infection
qic(month, n, days,
data = hospital_infections,
facets = ~ infection,
chart = 'u',
multiply = 10000,
title = 'Hospital acquired infections in the Capital Region of Denmark',
ylab = 'Cases per 10,000 risk days',
xlab = 'Month')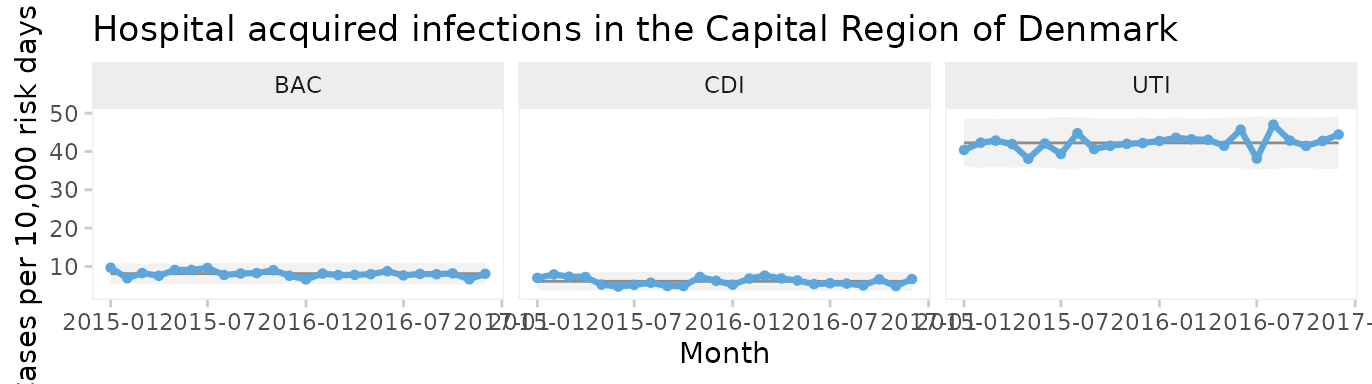
Now each infection has its own facet. We see that all three infections appear to be predictable and that UTI is the most common infection.
But since these data come from six very different hospitals, we should also facet by hospital.
Two-way faceted U chart by infection and hospital
qic(month, n, days,
data = hospital_infections,
facets = infection ~ hospital,
chart = 'u',
multiply = 10000,
scales = 'free_y',
x.angle = 45,
title = 'Hospital acquired infections in the Capital Region of Denmark',
ylab = 'Cases per 10,000 risk days',
xlab = 'Month')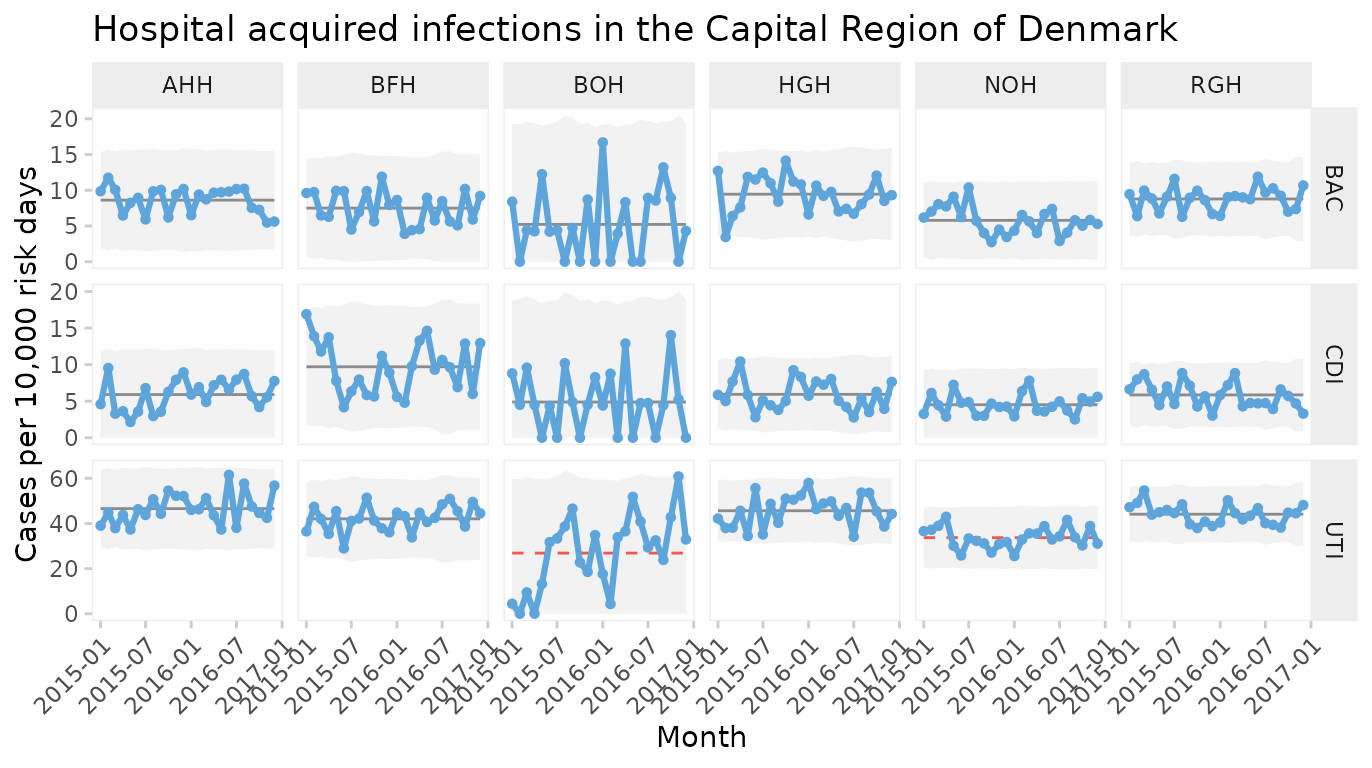
This plot makes it easy to display the differences between both hospitals and types of infection. Non-random variation is present in UTI rates of two hospitals (BOH, NOH).
Note the use of individual y axes to better visualise variation over time and the rotated x axis labels to avoid overlapping labels.
Funnels plot of infection rates by hospital
Processes containing only common cause variation over time may be aggregated and compared across other units than time. When data have no natural time order, i.e., when the x variable is categorical, the data points are not connected by lines and runs analysis is not performed. To produce a funnel plot of infections by hospital, we filter data from a recent stable period and reorder the x variable by size.
hai_2016 <- hospital_infections %>%
filter(month >= '2016-07-01') %>%
mutate(hospital = reorder(hospital, days))
qic(hospital, n, days,
data = hai_2016,
facets = ~ infection,
ncol = 1,
scales = 'free_y',
chart = 'u',
multiply = 10000,
decimals = 1,
show.labels = TRUE,
title = 'Hospital acquired bacteremia 2016 (U funnel chart)',
ylab = 'Cases per 10,000 risk days',
xlab = 'Hospital')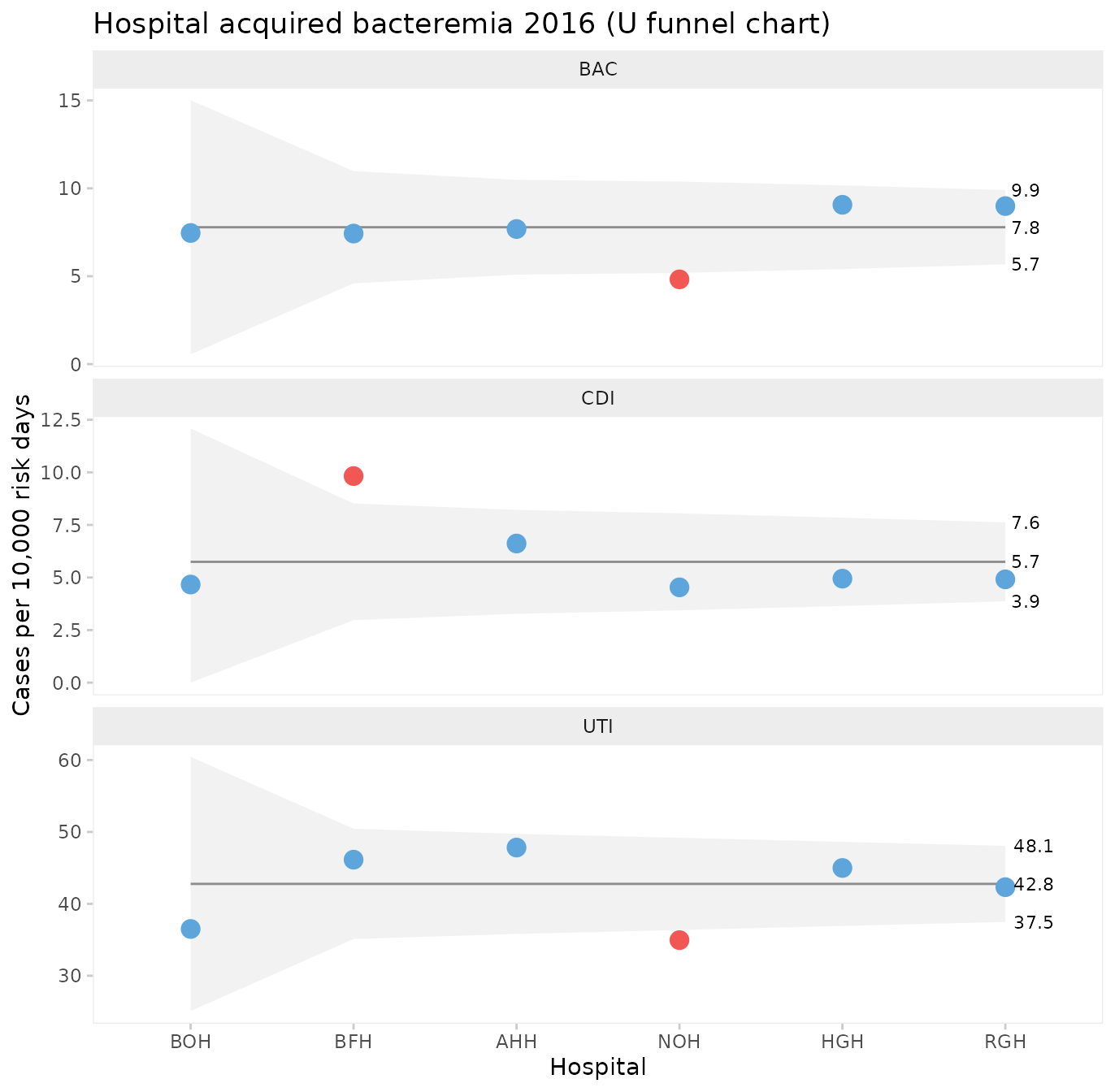
One hospital, NOH, has unusually few bacteremias and urinary tract infections compared to the other hospitals. Another hospital, BFH, has unusually many Clostridium difficile infections. The other hospitals are indistinguishable from each other with respect to the hospital infection rates.
What can we learn from NOH and BFH? It is important to stress that data presented in funnel plots should be used for learning rather than for judgement. While it may be interesting for some in need of a “case” to point fingers at the good, the bad, and the ugly, the full power of SPC will only be released when data are used for learning and improvement.
Case 5: Prime charts for count data with very large sample sizes
P and U charts with very large sample sizes sometimes produce narrow 3-sigma limits with most of the data points outside the limits even when the process is stable.
The nhs_accidents dataset contains the number of
emergency patients seen within 4 hours of attendance. The sample sizes
are very large (> 250,000). See ?nhs_accidents for
details.
head(nhs_accidents)
#> i r n
#> 1 1 266501 280443
#> 2 2 264225 276823
#> 3 3 276532 291681
#> 4 4 281461 296155
#> 5 5 269071 282343
#> 6 6 261215 275888When plotted on a P chart, the 3-sigma limits appear too narrow.
qic(i, r,
n = n,
data = nhs_accidents,
chart = 'p',
decimals = 3,
title = 'Proportion of patients seen within 4 hours of attendance (P chart)',
ylab = NULL,
xlab = 'Week #')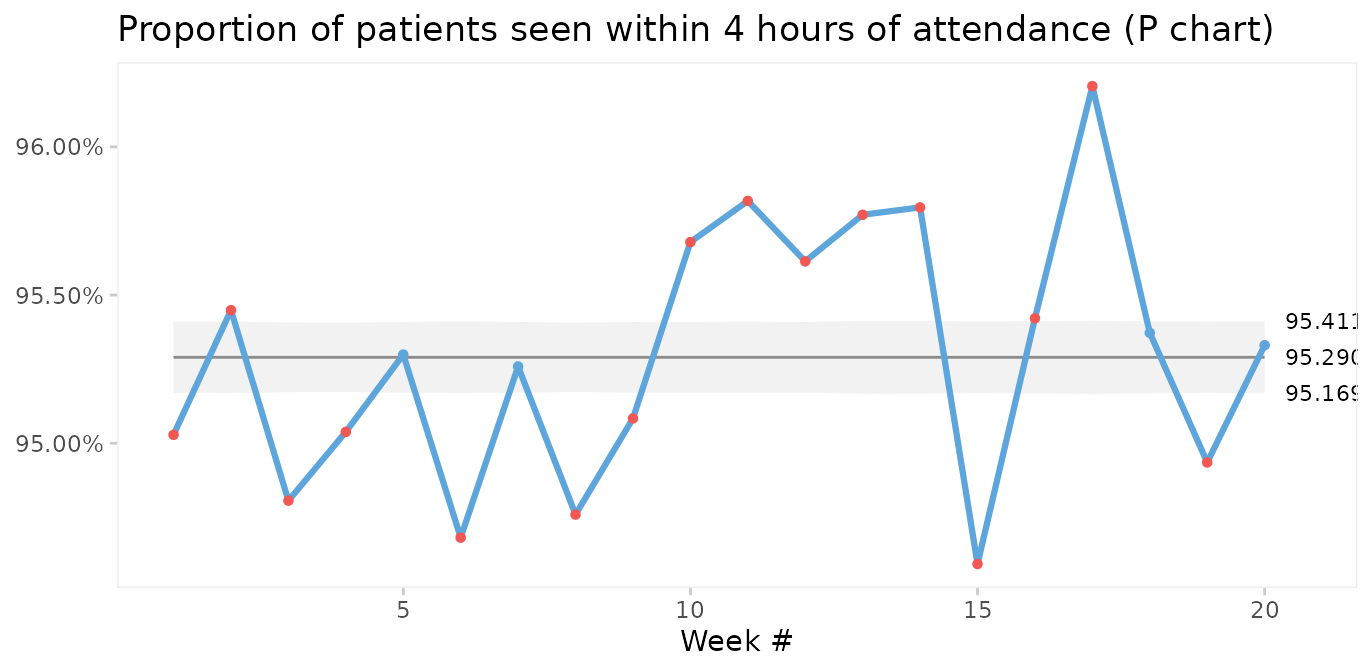
This is called over-dispersion, and happens sometimes because data in practice rarely come from truly binomial or poisson distributions. When the sample sizes are small, this is not a problem. But as sample sizes increase (> 1000) it becomes apparent that the assumptions of constant proportions or rates between subgroups are not true.
A simple test for over-dispersion is to apply an I chart. If the I chart gives 3-sigma limits that are very different from the U or P chart, it is a signal that the underlying probability model of the U or P chart may not be correct.
qic(i, r,
n = n,
data = nhs_accidents,
chart = 'i',
decimals = 3,
title = 'Proportion of patients seen within 4 hours of attendance (I chart)',
ylab = NULL,
xlab = 'Week #')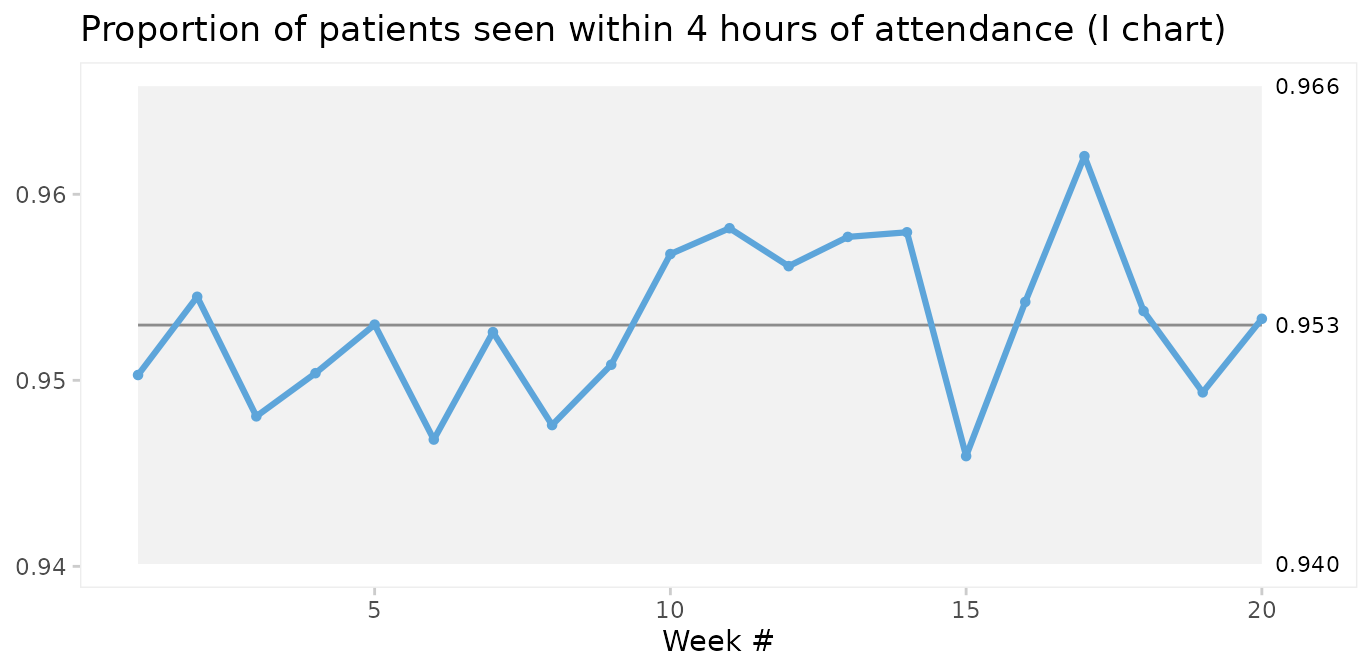
In fact, since the I chart estimates 3-sigma limits based on the observed within subgroup variation in data rather than an assumed probability model, it is sort of like the Swiss army knife of SPC. Therefore, the I chart may be used when the true probability model of data is unknown.
However, the I chart does not account for varying sample sizes and may give false signals when sample sizes vary significantly. Laney proposed an elegant solution that incorporates both within and between subgroup variation in the calculation of 3-sigma limits. This is what P’ (P prime) and U’ (U prime) charts are for. See Laney 2002 for details.
qic(i, r,
n = n,
data = nhs_accidents,
chart = 'pp',
decimals = 3,
title = 'Proportion of patients seen within 4 hours of attendance (P\' chart)',
ylab = NULL,
xlab = 'Week #')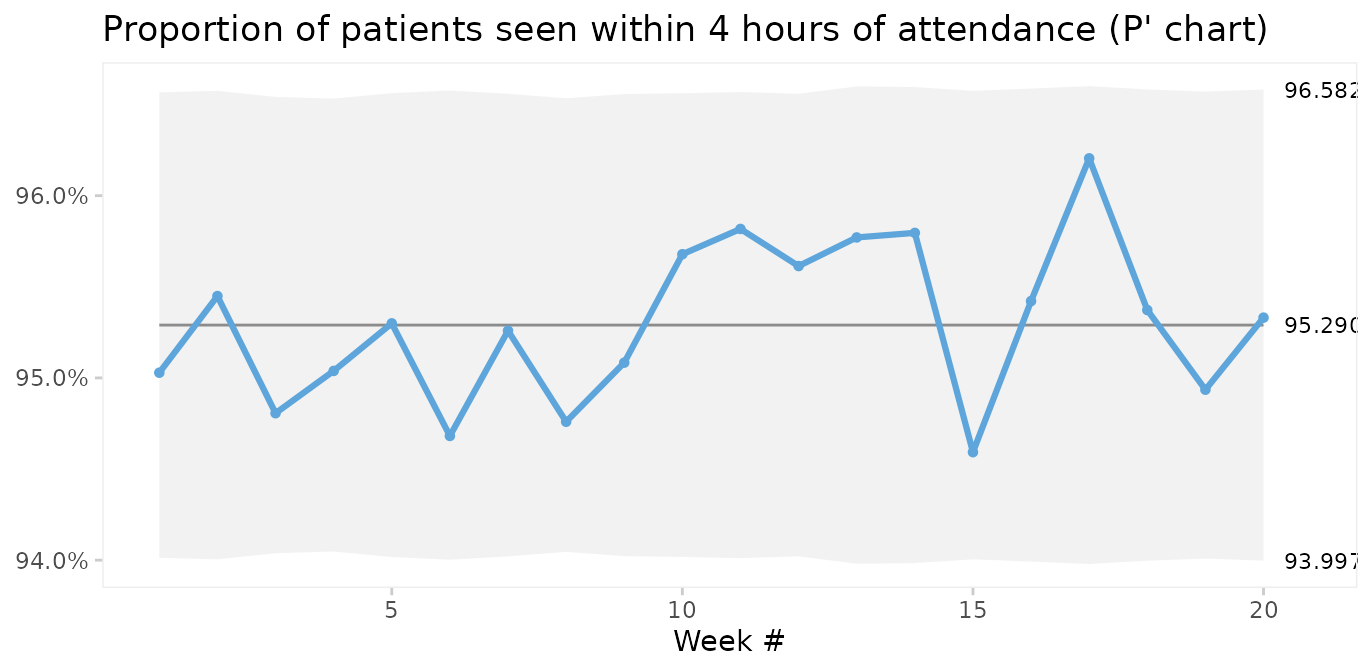
Laney notes that when over-dispersion is not present, prime charts will give the same results as traditional charts, and recommends always to use prime charts for proportions and rates.
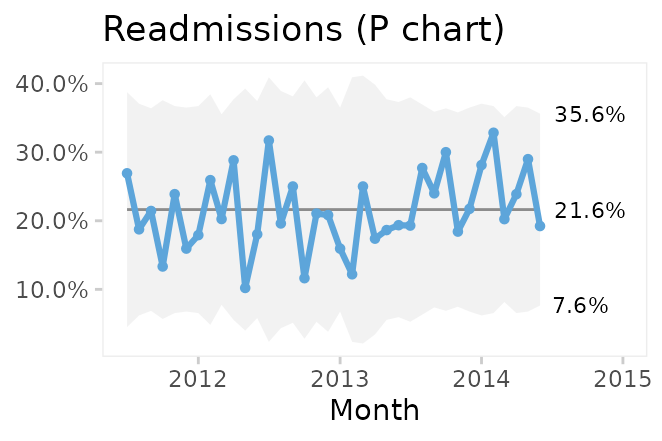
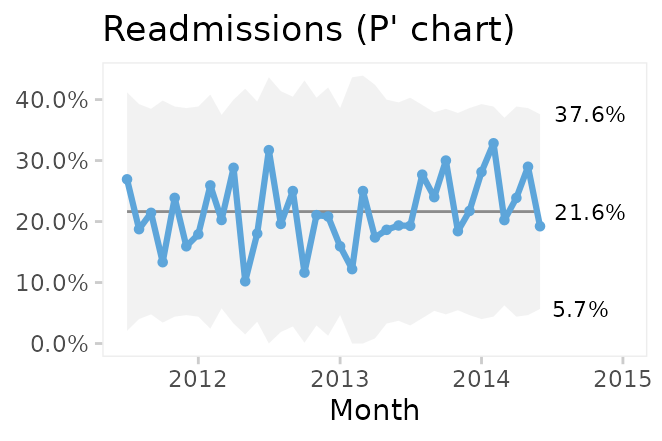
Comparing P and P’ charts on readmission rates from the
cabg dataset we find that while the 3-sigma limits in the
P’ chart are a little wider, the two charts reach similar
conclusions.
Conclusion
qic() from qicharts2 provides a simple
interface for constructing statistical process control charts for time
series data.
The default chart is a run chart, which tests for non-random
variation in data over time using the Anhøj rules for unusually long
runs and unusually few crossings. The Anhøj rules are most useful for
detection of moderate, persistent shifts. To detect larger, possibly
transient, shifts, control charts are useful. qic() employs
11 types of control charts for different types of data.
Since runs analysis based on the Anhøj rules makes no assumptions about the distribution of data, a run chart is the recommended starting point of any analysis of time series data. If the run chart finds random variation only, a control chart may then be used to identify transient shifts in data or to establish the natural process limits to be expected in the future.
References
Donald J. Wheeler (2000). Understanding Variation – The Key to Managing Chaos, second edition. SPC Press.
Jacob Anhøj, Anne Vingaard Olesen (2014). Run Charts Revisited: A Simulation Study of Run Chart Rules for Detection of Non-Random Variation in Health Care Processes. PLoS ONE 9(11): e113825.
Jacob Anhøj (2015). Diagnostic Value of Run Chart Analysis: Using Likelihood Ratios to Compare Run Chart Rules on Simulated Data Series. PLoS ONE 10(3): e0121349.
Donald J. Wheeler (2010). Understanding Statistical Process Control, third edition. SPC Press.
Douglas C. Montgomery (2009). Statistical Quality Control – A Modern Introduction, sixth edition. John Wiley & Sons.
Lloyd S. Nelson (1982). Control Charts for Individual Measurements. Journal of Quality Technology 14(3), 172-173.
David B. Laney (2002). Improved control charts for attributes. Quality Engineering, 14(4), 531-537.
Appendix 1: Calculating 3-sigma limits
The functions for calculating 3-sigma limits with
qicharts2 are based on the formulas provided by Montgomery
(Montgomery 2009). Laney’s correction factor for prime charts is from
Laney 2002.
The general model for a control charts is
where is the weighted average of the sample statistic and is the weighted sample standard deviation.
The procedure for calculating depends on the type type of data involved:
I: , , sample average, average moving range of successive observations.
MR: , average moving range (no lower 3-sigma limit).
Xbar: , constant depending on the sample size, weighted sample standard deviation.
S: , weighted sample standard deviation, and constants depending on the sample size.
C: , average number of defects.
U: , average number of defects per unit, size of inspection unit.
P: , average number of defectives, sample size.
G: , average number of opportunities between events.
Notes
I charts use the correction suggested by Nelson by excluding moving ranges above the upper range limit from calculations of the 3-sigma limits (Nelson 1982).
Runs analysis are not performed on MR charts since individual data points are correlated.
3-sigma limits for the T chart for time between rare events are calculated by applying an I chart to transformed data () and back transforming the 3-sigma limits ().
In prime charts, the calculated standard deviation is multiplied by Laney’s correction factor, which is the average moving range of standardised y values divided by the constant 1.128 (Laney 2002).
Since the count data on a G chart are usually highly skewed, the centre line of the G chart is the median rather than the mean. This way the application of the Anhøj rules is still valid.
Appendix 2: Critical values for longest run and number of crossings
n <- 10:100
x <- data.frame(
`Number of useful observations` = n,
`Upper limit for longest run` = round(log2(n) + 3),
`Lower limit for number of crossings` = qbinom(0.05, n - 1, 0.5),
check.names = FALSE)
knitr::kable(x)| Number of useful observations | Upper limit for longest run | Lower limit for number of crossings |
|---|---|---|
| 10 | 6 | 2 |
| 11 | 6 | 2 |
| 12 | 7 | 3 |
| 13 | 7 | 3 |
| 14 | 7 | 4 |
| 15 | 7 | 4 |
| 16 | 7 | 4 |
| 17 | 7 | 5 |
| 18 | 7 | 5 |
| 19 | 7 | 6 |
| 20 | 7 | 6 |
| 21 | 7 | 6 |
| 22 | 7 | 7 |
| 23 | 8 | 7 |
| 24 | 8 | 8 |
| 25 | 8 | 8 |
| 26 | 8 | 8 |
| 27 | 8 | 9 |
| 28 | 8 | 9 |
| 29 | 8 | 10 |
| 30 | 8 | 10 |
| 31 | 8 | 11 |
| 32 | 8 | 11 |
| 33 | 8 | 11 |
| 34 | 8 | 12 |
| 35 | 8 | 12 |
| 36 | 8 | 13 |
| 37 | 8 | 13 |
| 38 | 8 | 14 |
| 39 | 8 | 14 |
| 40 | 8 | 14 |
| 41 | 8 | 15 |
| 42 | 8 | 15 |
| 43 | 8 | 16 |
| 44 | 8 | 16 |
| 45 | 8 | 17 |
| 46 | 9 | 17 |
| 47 | 9 | 17 |
| 48 | 9 | 18 |
| 49 | 9 | 18 |
| 50 | 9 | 19 |
| 51 | 9 | 19 |
| 52 | 9 | 20 |
| 53 | 9 | 20 |
| 54 | 9 | 21 |
| 55 | 9 | 21 |
| 56 | 9 | 21 |
| 57 | 9 | 22 |
| 58 | 9 | 22 |
| 59 | 9 | 23 |
| 60 | 9 | 23 |
| 61 | 9 | 24 |
| 62 | 9 | 24 |
| 63 | 9 | 25 |
| 64 | 9 | 25 |
| 65 | 9 | 25 |
| 66 | 9 | 26 |
| 67 | 9 | 26 |
| 68 | 9 | 27 |
| 69 | 9 | 27 |
| 70 | 9 | 28 |
| 71 | 9 | 28 |
| 72 | 9 | 29 |
| 73 | 9 | 29 |
| 74 | 9 | 29 |
| 75 | 9 | 30 |
| 76 | 9 | 30 |
| 77 | 9 | 31 |
| 78 | 9 | 31 |
| 79 | 9 | 32 |
| 80 | 9 | 32 |
| 81 | 9 | 33 |
| 82 | 9 | 33 |
| 83 | 9 | 34 |
| 84 | 9 | 34 |
| 85 | 9 | 34 |
| 86 | 9 | 35 |
| 87 | 9 | 35 |
| 88 | 9 | 36 |
| 89 | 9 | 36 |
| 90 | 9 | 37 |
| 91 | 10 | 37 |
| 92 | 10 | 38 |
| 93 | 10 | 38 |
| 94 | 10 | 39 |
| 95 | 10 | 39 |
| 96 | 10 | 39 |
| 97 | 10 | 40 |
| 98 | 10 | 40 |
| 99 | 10 | 41 |
| 100 | 10 | 41 |